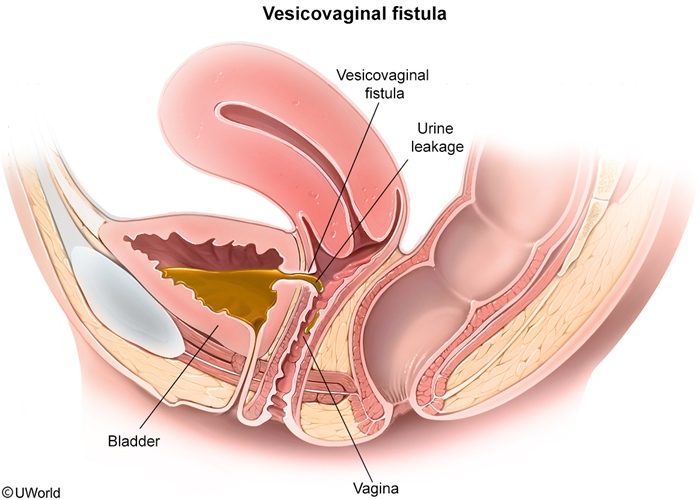
Vesicovaginal fistula
| Vesicovaginal fistula | |
|---|---|
| Risk factors | Pelvic surgery Pelvic irradiation Prolonged labor/childbirth trauma Genitourinary malignancy |
| Clinical features | Painless, continuous urine leakage from the vagina |
| Diagnostic studies | Physical examination Dye test Cystourethroscopy |
This patient's continuous painless urine leakage is most likely due tovesicovaginal fistula after her recent pelvic surgery. In industrialized countries, most urogenital fistulas are due to pelvic surgery or radiotherapy for cancer. Fistulas may result from occult bladder injury during pelvic surgery or from tissue ischemia due to excessive surgical dissection. Urinary incontinence (eg, persistent uncontrolled leakage) into the vagina may present within a month after surgery.
The diagnosis is made clinically by visualization of urine leaking into the vagina. Sometimes a small area of granulation tissue or a hole may be seen. Dye tests and/or cystourethroscopy may be performed to identify a small fistula that is difficult to detect on visual inspection. Cystitis may be a complication, and urinalysis may indicate infection (positive leukocyte esterase/nitrites, bacteriuria, pyuria), as seen in this patient. Bladder catheterization in the immediate postoperative period allows a small fistula to heal. Otherwise, surgical correction is indicated.
Methylene blue is instilled into the bladder to diagnose urinary incontinence due to a vesicovaginal fistula. The test is positive if a tampon placed in the vagina becomes blue after the dye is instilled in the bladder.