uti in pregnancy
- related: OBGYN
- tags: #obgyn
This pregnant patient in the third trimester has features of cystitis (eg, urinary frequency, suprapubic tenderness). The additional features of high-grade fever, peripheral leukocytosis, and marked pyuria suggest early acute pyelonephritis (despite the absence of costovertebral tenderness). Pyelonephritis during pregnancy causes an increased risk for complications such as acute respiratory distress syndrome and pulmonary edema. Adverse pregnancy outcomes include preterm labor and low birth weight. Pregnant women, particularly those in the later stages of pregnancy, are at increased risk for pyelonephritis due to anatomical changes in the urinary tract and immunosuppression caused by pregnancy.
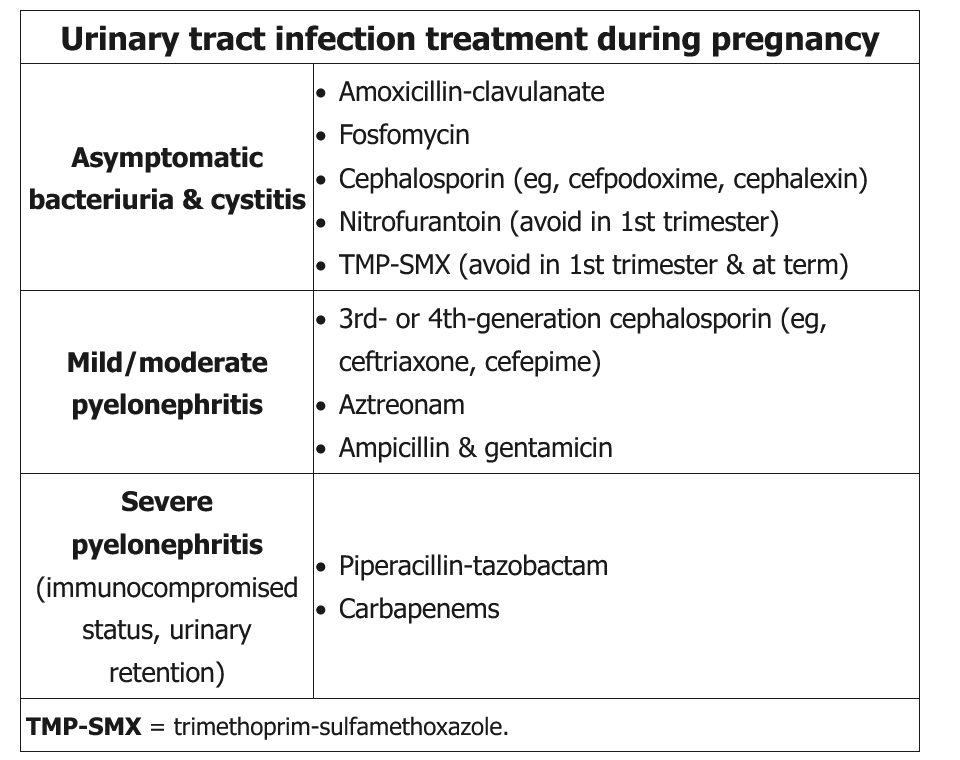
Current guidelines recommend inpatient admission and intravenous antibiotics until the patient is afebrile and demonstrates symptomatic improvement for 24 to 48 hours (Choices A, D, and E). Escherichia coli most commonly causes pyelonephritis during pregnancy, but other gram-negative bacteria and gram-positive organisms (eg, group B Streptococcus) may cause bacteriuria during pregnancy.
Intravenous ceftriaxone is the treatment of choice for acute pyelonephritis in pregnancy given its efficacy and low side effect profile. Aminoglycosides are not considered first-line agents as prolonged exposure has been associated with fetal ototoxicity.