tinnitus
- related: ENT
- tags: #note
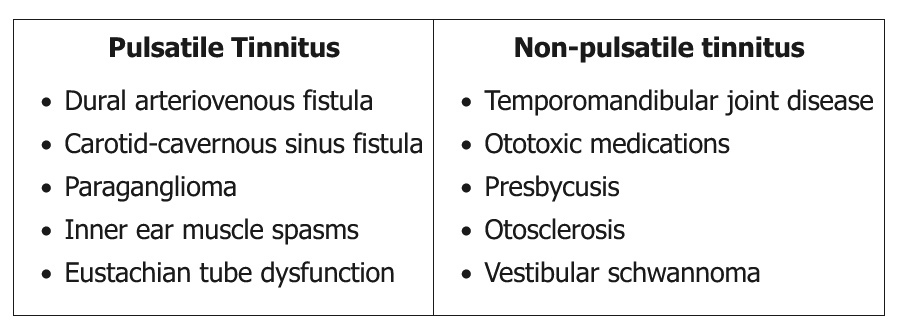
Tinnitus is defined as a sound perception within the head or ears that can be buzzing, ringing, or hissing. Pulsatile tinnitus usually implies a significant underlying vascular pathology, while non-pulsatile tinnitus tends to be non-vascular (causes listed in the above table). Pulsatile tinnitus usually requires a thorough investigation with an ENT consult and brain imaging. Non-pulsatile tinnitus is usually due to dysfunction within the auditory system (cochlear end-organ, cochlear nerve, brainstem, and auditory cortex). Tinnitus is often a sign of sensorineural hearing loss, although most patients do not complain of hearing loss.
This patient's tinnitus (high-pitched ringing, non-pulsatile, continuous, not affected by position) suggests an origin within the auditory system. Patients with non-pulsatile tinnitus believed to originate from the auditory pathways require initial audiometric testing to detect asymmetry between the two ears and abnormalities in the middle ear, cochlea, or brainstem. Further work-up and treatment is based upon these findings.
Both nonsteroidal anti-inflammatory drugs and angiotensin converting enzyme inhibitors have been linked to tinnitus, but the association is unclear. Pending the results of the audiometric evaluation, a trial of discontinuation of ibuprofen and substitution for enalapril may be indicated.
Magnetic resonance angiography would be indicated in patients who present with a vascular origin of the tinnitus such as history of pulsatile, intermittent, or position-dependent tinnitus; or a bruit in the head and neck region.
Non-contrast CT helps evaluate for intracranial hemorrhage and many cortical lesions, but contrast head CT is required to evaluate patients with pulsatile tinnitus for tumors such as paraganglioma. This patient has non-pulsatile tinnitus with a benign examination and would not require head CT.