testicular pain ddx
- related: Urology
- tags: #note
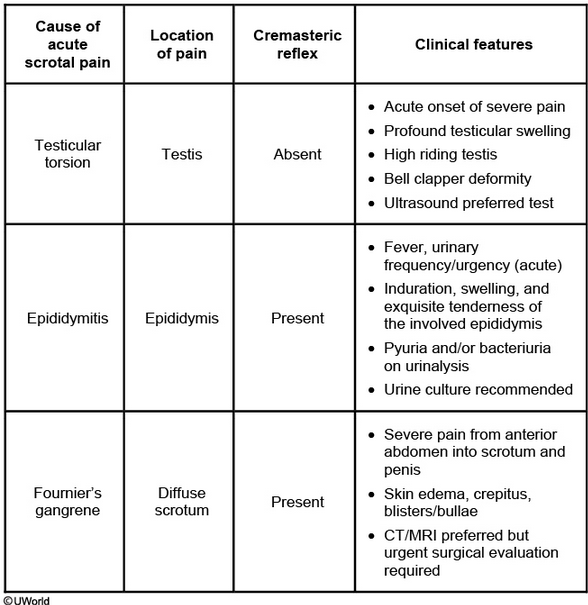
This patient has refractory scrotal pain despite adequate therapy for epididymitis, and he should be evaluated for more emergent causes (eg, testicular torsion, testicular abscess, or testicular infarction). History and physical examination often cannot differentiate between these diagnoses. For instance, although an abscess usually demonstrates fluctuance, the examination may not always show this. Similarly, although testicular torsion (associated with an absent cremasteric reflex) is more common in boys age ≤12, it can also occur in adult men.
Despite receiving antibiotic therapy, this patient has persistent left-sided scrotal pain and swelling that is decreased with sac elevation (consistent with but not specific to epididymitis, and uncommon in testicular torsion) along with an equivocal cremasteric reflex. He needs immediate evaluation by a urologist and ultrasonography or radionuclide scrotal imaging to identify the cause of his pain and to determine the need for surgical intervention. Although he was initially diagnosed with epididymitis, this particular patient was eventually found to have testicular cancer, which can occasionally present as acute testicular pain.