-
Arrythmia
Arrythmia
- Keywords: Cardiology General
- tag: #note
Inherited Arrhythmia Syndromes
Patients younger than age 40 years with unexplained SCD, unexplained near drowning, or recurrent exertional syncope, who do not have ischemic or other structural heart disease, should be evaluated for inherited arrhythmia syndromes. Additionally, unexplained premature death (age <35 years) or sudden death in a
-
Multifocal Atrial Tachycardia
Multifocal Atrial Tachycardia
- related: Medicine, Cardiology, tachycardia
- tag: #note
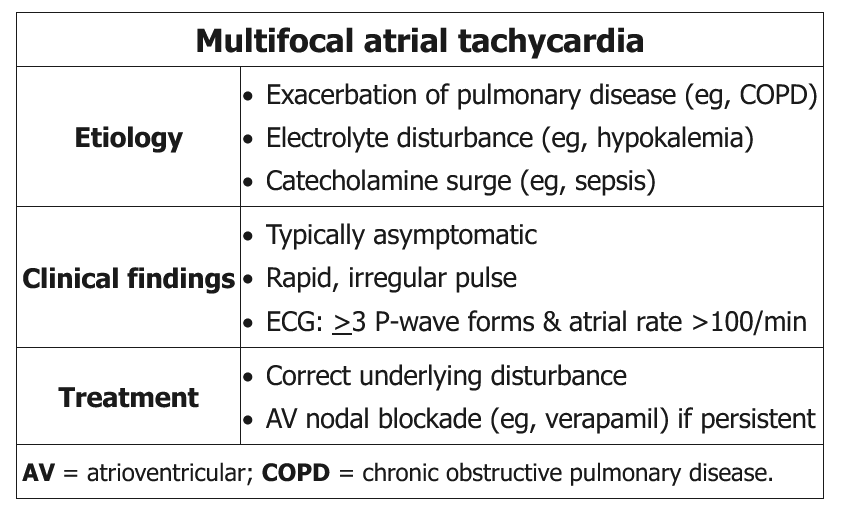
Multifocal atrial tachycardia (MAT) is an irregularly-irregular supraventricular tachycardia (SVT) characterized by the presence of 3 or more ectopic atrial pacemaking foci.
MAT occurs more commonly in patients with COPD, hypoxemia, and underlying pulmonary dysfunction. Other
-
Atrial Fibrillation
atrial fibrillation
- related: tachycardia, Arrythmia, Cardiology
- tag: #note
epidemiology
- most common sustained arrhythmia
- affect more than 33 million persons worldwide
- Lifetime risk for atrial fibrillation is 25% in patients older than 40 years.
- Incidence is strongly associated with and increases with age.
- 10% of persons older than 80 years.
- fivefold increased risk for stroke
- increased risk for heart failure and dementia
- Among patie
-
Sinus Tachycardia
sinus tachycardia
- related: Medicine, Cardiology, tachycardia
- tag: #note
Causes
- sepsis
- fever
- usually persistent
- volume
- Anemia
- Dehydration
- usually persistent
- stress
- Pain
- Anxiety
- ACS
- HF
- others
- Withdrawal
- Intoxication
- TSH
Inappropriate sinus tachycardia
- IST
- pt: women in 30s-40s
- elevated resting heart rate
- exaggerated increase with light activity
- decreased rate with sleep
- treatment:
- remova
-
SVT
SVT
- related: tachycardia
- tags: #note
SVTs are rapid heart rhythms that arise from the atrium or require conduction through the AV node. Atrial fibrillation and atrial flutter are technically SVTs, although the term generally pertains to paroxysmal SVTs. SVTs can affect all age groups but frequently occur in younger patients. Prevalence is higher in women than in men. SVTs usually occur in the absence of structural heart disease, although echocardiography shou
-
Atrial Flutter
atrial flutter
- related: tachycardia
- tags: #note
Atrial Flutter
Related Question
- Question 12
Atrial flutter is an organized macro-reentrant tachycardia with discrete regular atrial activity on ECG, usually with a rate of 250/min to 300/min. Typical atrial flutter is characterized electrocardiographically by a sawtooth pattern with inverted flutter waves in leads II, III, and aVF and positive flutter waves in lead V1 (**[Figure 14](https://mksap18.
-
PVC
PVC
- related: tachycardia
- tags: #note
Premature ventricular contractions (PVCs) occur in up to 75% of healthy persons.
Symptoms
Symptoms include palpitations or the perception of skipped beats. Forceful beats are caused by increased cardiac filling during the pause following the PVC. PVCs are more common in patients with hypertension, left ventricular hypertrophy, previous myocardial infarction, and other forms of structural heart disease, such as
-
Vtach
vtach
- related: tachycardia
- tags: #note
EKG characteristics
In adult patients with structural heart disease, 95% of wide-complex tachycardias are VT. Several important clinical and ECG features can distinguish VT from other conditions. Wide-complex tachycardias that are positive in lead aVR, have a QRS morphology that is concordant in the precordial leads, have QRS morphology other than typical right or left bundle branch block, and exhibit