supratherapeutic INR
- related: Hemeonc
- tags: #hemeonc
Patients on warfarin therapy are at risk for elevated INR due to drug interactions, vitamin K deficiency, and superimposed conditions (eg, diarrhea, fever, liver disease, heart failure). Impaired cognition, depression, or low literacy can also lead to elevated INR due to incorrect warfarin dosing.
The initial approach to elevated INR depends on the following:
- Degree of elevation
- Presence of active bleeding
- Patient's bleeding risk
- Indications for continued warfarin therapy after the episode resolves
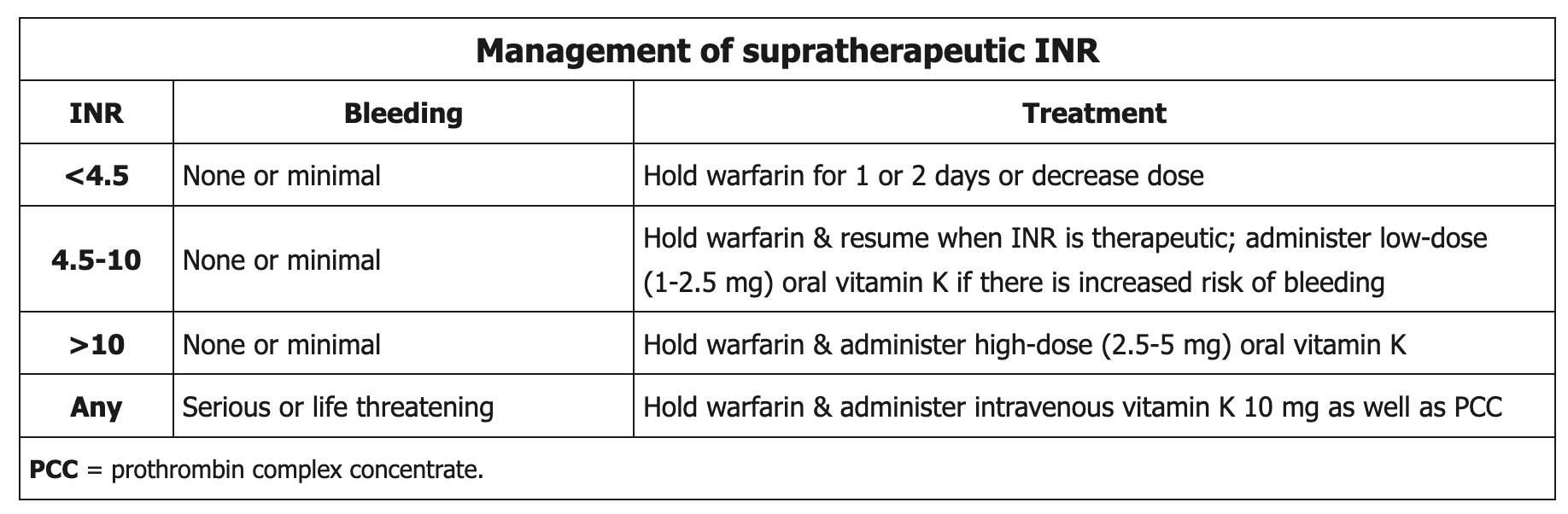
Patients with INR <4.5 who have no significant bleeding can be managed by holding warfarin for 1-2 doses and/or slightly reducing the maintenance dose. INR 4.5-10 is managed similarly if no bleeding is present; those with increased bleeding risk (eg, older age, history of bleed) may also be treated with low-dose oral vitamin K. Patients with INR >10 who have no concurrent bleeding require temporary warfarin cessation and high-dose oral vitamin K* (as risk for major bleed is 10%-20%). Oral vitamin K is preferred as it is as effective as intravenous (IV) vitamin K in lowering INR within 48 hours and is associated with a lower risk of anaphylaxis.