Subclinical hyperthyroidism
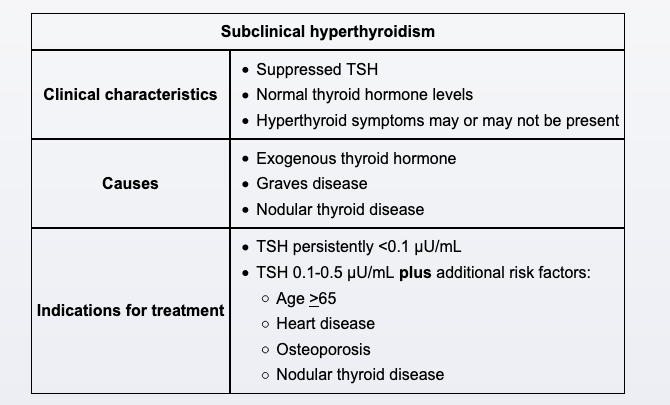
Subclinical hyperthyroidism is defined as low TSH with normal thyroid hormone concentrations. Transient fluctuations in thyroid markers can be seen (particularly with acute illness), but patients who have persistently suppressed TSH levels warrant further evaluation. This patient has a diffusely increased radioiodine uptake consistent with Graves disease, with worsening of thyroid function test results possibly due to iodinated dye administration during his recent cardiac catheterization. Other common causes of subclinical hyperthyroidism include exogenous thyroid hormone, nodular thyroid disease (thyroid adenoma or toxic multinodular goiter), and inflammatory thyroiditis (eg, silent thyroiditis, subacute [de Quervain] thyroiditis).
Severe TSH suppression (<0.1 µU/mL) is associated with a higher risk for progression to overt hyperthyroidism and warrants treatment. Patients with mildly suppressed TSH levels (0.1-0.5 µU/mL) often experience spontaneous remission and can usually be monitored with periodic thyroid function tests. However, those with increased risk for complications due to age (>65) or comorbid conditions (eg, heart disease, osteoporosis) warrant consideration for treatment with antithyroid medication or radioactive iodine. In light of this patient's TSH <0.1 μU/mL, age >65, and comorbid coronary artery disease, treatment should be offered at this time.