Secondary Hypertension
Causes
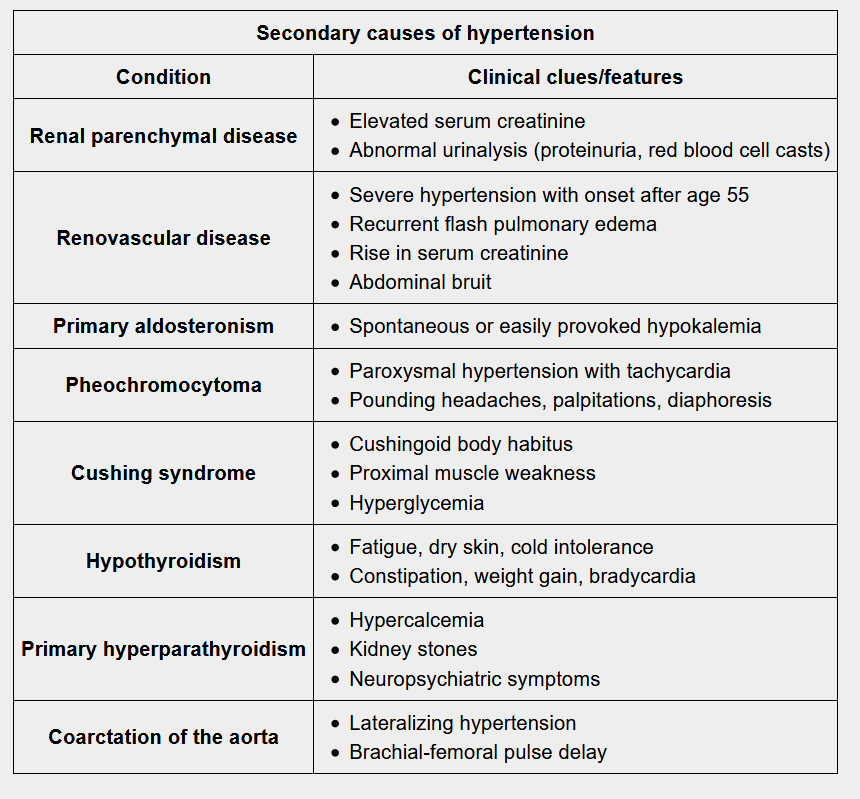
Often these patients have a history of hypertension refractory to the maximal dosage of several drugs.
Renal artery stenosis is more common in female patients less than 25 years of age (fibromuscular dysplasia) and in patients over the age of 50 (atherosclerosis).
The presence of a persistent abdominal bruit that lateralizes to one side is highly suggestive of renovascular hypertension (sensitivity of 40%, specificity of 99%).
An acute increase in serum creatinine by ≥30% following initiation of an ACE inhibitor or ARB in a patient that is not hypovolemic is highly suggestive of renovascular hypertension.
While fibromuscular dysplasia most commonly involves the renal arteries, it can also involve the carotid and vertebral arteries. Thus, patients can present with headache, pulsatile tinnitus, and neck pain as well as manifestations of CNS ischemia (e.g. amaurosis fugax, transient ischemic attack).
Combination oral contraceptive pills (OCPs) are more likely to cause hypertension in women over 35 years of age, obese women, and in patients with a history of long-term OCP use.
Pheochromocytomas occur more commonly in younger patients with a history of endocrine tumors.
Aortic coarctation is more common in patients with Turner syndrome, especially on test questions.
To remember some common medications which cause elevations in blood pressure, it may help to recall the mnemonic GONADS:
- Glucocorticoids
- OCPs (oral contraceptive pills)
- NSAIDs (non-steroidal anti-inflammatory agents)
- Antidepressants (particularly SNRIs)
- Decongestants (pseudoephedrine)
- Stimulants (methylphenidate, amphetamines)
| Secondary hypertension treatment depends on etiology. Cause | Treatment |
|---|---|
| Renal parenchymal disease | ACE inhibitor or ARB to delay progression |
| Renal artery stenosis | Angioplasty, stent placement; ACE inhibitoror ARB if one-sided (contraindicated in bilateral renal artery stenosis because renal perfusion and GFR will decrease) |
| Combination oral contraceptives | Stop OCP, change to progestin-only pill or intramuscular medroxyprogesterone |
| Pheochromocytoma | Control hypertension pharmacologically (phenoxybenzamine x 10 to 14 days, then add propranolol 1 to 2 days before surgery); then adrenalectomy after 10 to 14 days of alpha blockade |
| Primary hyperaldosteronism (Conn syndrome) | Aldosterone antagonists (spironolactone, eplerenone) and surgical resection |
| Excess glucocorticoids (Cushing syndrome) | Treat underlying cause and reduce exogenous steroids |
| Aortic coarctation | Surgical correction |
| Hyperparathyroidism/hypercalcemia | Hydration |