Scoliosis
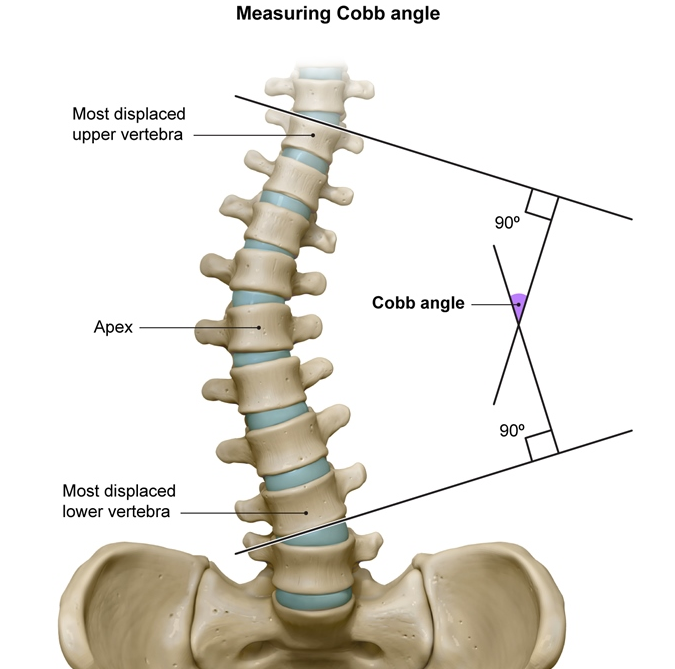
Although scoliometry helps to predict patients with clinically significant scoliosis, the results are user-dependent and nonspecific. Therefore, concerning scoliometer findings require further evaluation with posteroanterior and lateral x-rays. Cobb angle measures spine curvature on x-ray and is the gold standard for determining diagnosis and treatment of scoliosis. A Cobb angle <10 degrees, as seen in this patient, is considered a variant of normal. Therefore, no follow-up is needed unless new findings (eg, significant pain, neurologic symptoms) develop.
Conversely, patients with a Cobb angle ≥10 degrees have scoliosis. Scoliosis management depends on the risk for curve progression, with a larger Cobb angle signifying higher risk. Although observation or the use of a back brace is typically sufficient for low/medium risk curves (Choice B), severe scoliosis (Cobb angle ≥40 degrees) requires surgical evaluation for possible spinal fusion given the high risk for progression and future complications (eg, chronic back pain, pulmonary compromise) (Choice E). However, once puberty and skeletal maturity are complete, progression is typically minimal and treatment is not required unless severe deformity is present.
Skeletal maturity is reflected by the pubertal status, which can help in estimating the remaining growth potential. By Tanner stage 5, this postmenarcheal patient has completed puberty, undergone epiphyseal fusion, and likely reached her full growth potential. Because curve progression is minimal to nonexistent once skeletal maturity is reached, treatment is generally unnecessary, and no follow-up is required for mild/moderate scoliosis (Cobb angle <40 degrees, as in this patient).
Bracing the back helps reduce the risk of curve progression and the need for surgery in skeletally immature patients. However, it is ineffective in those with minimal growth potential, such as this patient who has completed puberty.
(Choice C) MRI of the spine can evaluate for congenital or neuromuscular causes of scoliosis if x-ray of the spine reveals concerning vertebral anomalies (eg, wedged or hemi-vertebrae, vertebral lucency), not seen in this case.
(Choice D) Although idiopathic scoliosis may have a hereditary component, genetic testing is expensive and unnecessary as x-ray determines diagnosis and management. This patient does not have scoliosis based on her Cobb angle and does not need further testing.