pulmonary auscultations
- related: Pulmonology
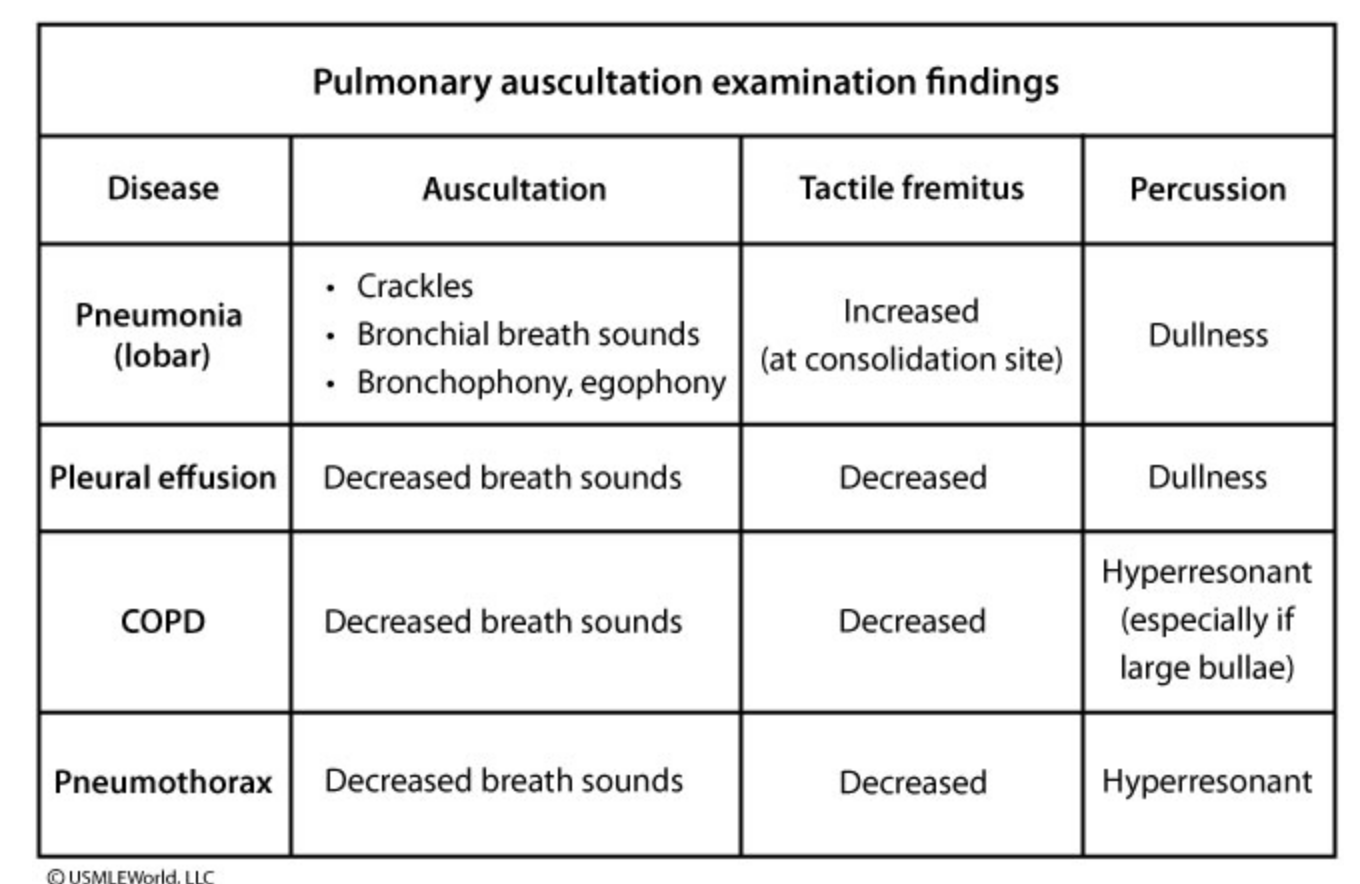
Palpable vibration felt on the chest wall is known as fremitus. Sound travels faster in solids (consolidation) than in an aerated lung, resulting in increased fremitus in pneumonia. However, pneumonia in the presence of an obstructed bronchus would not increase the fremitus. The presence of egophony, bronchophony, or whispered pectoriloquy also suggests a consolidative process. Presence of fluid or air outside the lung interrupts the transmission of sound, resulting in decreased fremitus in pleural effusion and pneumothorax.
Percussion reveals hyperresonance in patients with pneumothorax and dullness in patients with pleural effusions or pneumonia.
Patients with consolidative lung processes may also present with bronchial breath sounds due to over-transmission of sound over the chest wall. Over-transmission is due to airway patency leading to the affected area. Breath sounds are diminished or absent over a pleural effusion, pneumothorax, or bullae.
Late-inspiratory crackles are often found in restrictive lung diseases (pulmonary fibrosis). Wheezing, though often associated with bronchial asthma, can sometimes be provoked in healthy individuals with forced expiration. Similarly, several other diseases (eg, infection, vocal cord dysfunction, congestive heart failure) are associated with wheezing. Therefore, additional information is needed prior to making a diagnosis.
Presence of bronchial breath sounds, increased tactile fremitus, bronchophony, and dullness to percussion in this patient are suggestive of lobar pneumonia. However, the physical examination findings alone do not accurately diagnose pneumonia. A chest x-ray should therefore be ordered to confirm the diagnosis prior to initiating antibiotics.