perioperative management of chronic glucocorticoid
- related: Endocrine, Perioperative
- tags: #endocrine
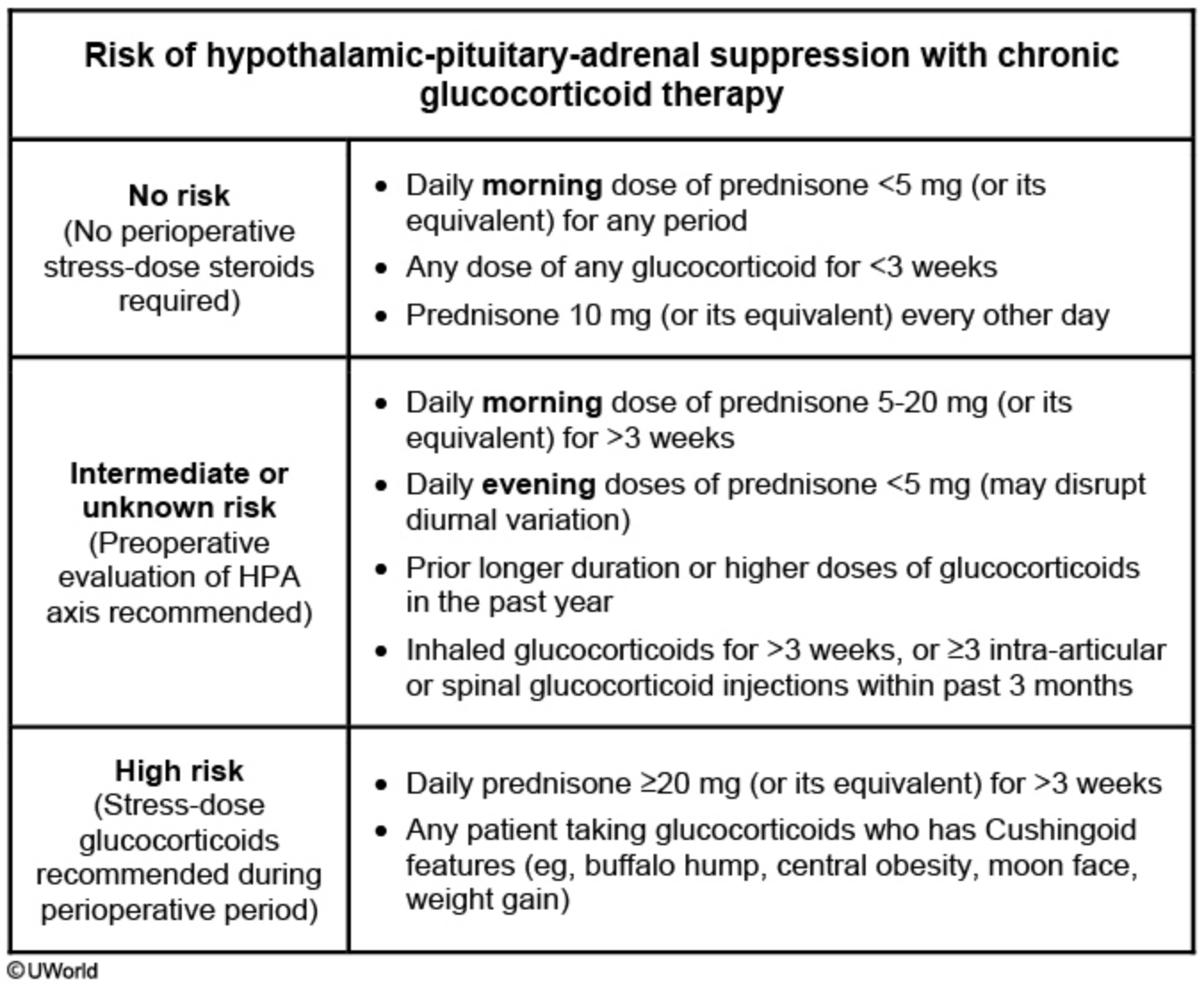
Suppression of adrenal function is likely to develop in patients receiving corticosteroids for a prolonged period. This is especially true for those who receive high doses and those who are dosed at night rather than during the morning hours. In addition, patients with a Cushingoid appearance are more likely to have a suppressed hypothalamic-pituitary-adrenal (HPA) axis. Patients treated with corticosteroids for <3 weeks are less likely to develop HPA suppression. More importantly, normal HPA axis function after corticosteroid use may not fully recover for up to 6-12 months after discontinuation of the medication. During the recovery period, a patient may be asymptomatic under normal conditions but can develop adrenal crisis during stressful situations such as severe illness or surgery.
An ACTH (cosyntropin) stimulation test is performed to determine whether stress-dose corticosteroids are necessary in patients at intermediate risk for HPA axis suppression. If the patient has a subnormal increase in cortisol level following ACTH stimulation, stress-dose corticosteroids must be given perioperatively.
A typical perioperative corticosteroid regimen for a major surgical procedure is hydrocortisone 100 mg intravenously during surgery followed by 50 mg every 8 hours for 24 hours with a rapid taper (generally 1-2 days) as the stress resolves.