parvo b19 in pregnancy
- related: parvo b19, Infections in Pregnancy
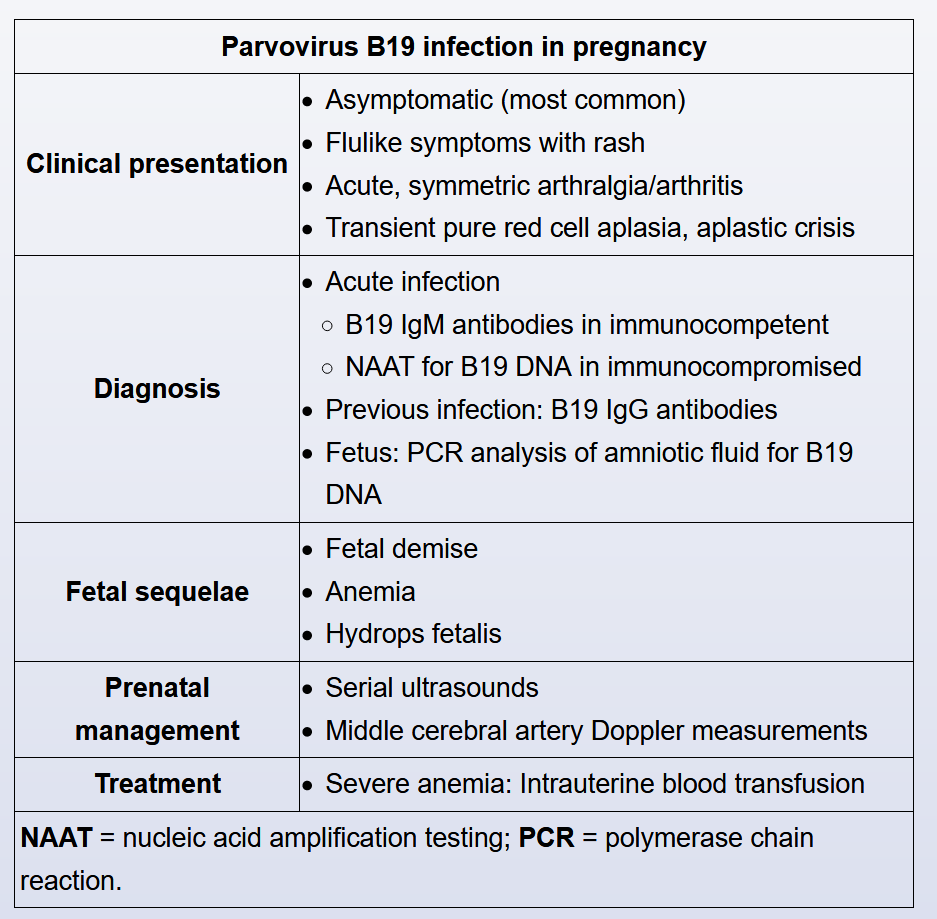
Parvovirus B19 infection is common in childhood, when clinical manifestations include fever followed by a "slapped cheek" appearance (eg, erythema infectiosum, or fifth disease). In immunocompetent adults, parvovirus B19 is typically a self-limiting, mild or asymptomatic infection; patients may have flulike symptoms; an erythematous lace-like rash; and symmetric, polyarticular arthralgias. Pregnant women also have mild or asymptomatic infections; however, their fetuses are at risk for devastating complications, including fetal anemia, hydrops fetalis, or fetal demise (Choice C).
Pregnant women with known exposures or symptoms suggestive of parvovirus B19 infection undergo serologic testing for the virus. Many immunocompetent adults show signs of previous infection, and therefore immunity, with parvovirus B19 (eg, +IgG antibodies and -IgM antibodies). Teachers have a higher risk of infection than the general population; however, if they have +IgG antibodies, there is no concern for acute parvovirus infection. The presence of IgM antibodies, which can be positive <10 days after exposure, indicates acute infection. If infection is strongly suspected despite negative IgM serologies, patients undergo PCR screening for maternal B19 DNA.
Parvovirus B19 is toxic to fetal red blood cell precursors and can lead to fetal anemia and hydrops fetalis. Pregnant women with active parvovirus B19 are at risk for fetal loss when infection occurs at <20 weeks gestation. Untreated, severe fetal hydrops can result in fetal demise; therefore, pregnant women with an active parvovirus infection undergo periodic ultrasonography to evaluate for anemia and hydrops fetalis. Severe anemia is treated with intrauterine fetal transfusion.