obesity management
- related: Endocrine
- tags: #endocrine
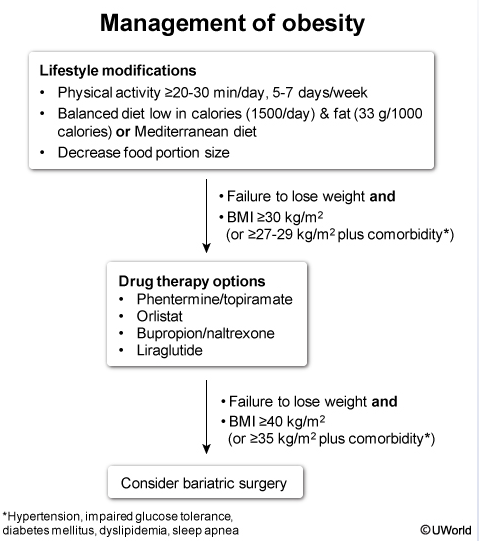
This patient has failed to improve with an adequate trial of dietary modification. In addition, she has continued to gain weight and now meets the definition of obesity (BMI >30 kg/m2). In light of the risk of obesity-related complications, pharmacologic therapy is indicated.
Initial medication options for patients with obesity are listed in the flow chart. Orlistat inhibits pancreatic lipases, resulting in decreased fat absorption. It is frequently chosen as a first-line drug due to its excellent safety profile and choice of low-dose (over-the-counter) and high-dose (prescription) options. However, orlistat is associated with significant gastrointestinal side effects (eg, diarrhea, bloating, fecal incontinence), and some patients may elect to start with another medication.
This patient's presentation is consistent with adverse effects from the anti-obesity medication orlistat. Orlistat is used for long-term treatment of obesity in patients with body mass index > 30 kg/m2or > 27 kg/m2 with comorbidities (eg, diabetes, dyslipidemia, hypertension). The drug inhibits pancreatic lipase to alter fat digestion, decrease fat absorption, and increase fecal fat excretion. As a result, patients with diet fat > 30% of total calories can develop symptoms similar to fat malabsorption disorders (eg, flatus, fecal incontinence, abdominal distension). A low-fat diet (< 30% total fat calories) can reduce these symptoms.
Orlistat can also decrease absorption of fat-soluble vitamins, and patients should take a daily multivitamin. Orlistat-induced fat malabsorption can also increase intestinal calcium binding, which leads to decreased available calcium to bind oxalate. This leads to increased oxalate absorption, increased urinary oxalate excretion, and possible calcium oxalate stones. As a result, orlistat should not be used in patients with history of calcium oxalate stones.