nephrolithiasis and pregnancy
This patient's paroxysmal, severe flank pain that radiates to the labia is likely due to nephrolithiasis. Other clinical features of nephrolithiasis include nausea, vomiting, dysuria, hematuria, and pyuria. During pregnancy, nephrolithiasis is most common in the second and third trimesters. An increase in urinary calcium excretion, urinary stasis, and decreased bladder capacity predispose pregnant patients to the development of nephrolithiasis. Additional risk factors include obesity, hyperparathyroidism, diabetes mellitus, irritable bowel syndrome, and a history of nephrolithiasis outside of pregnancy.
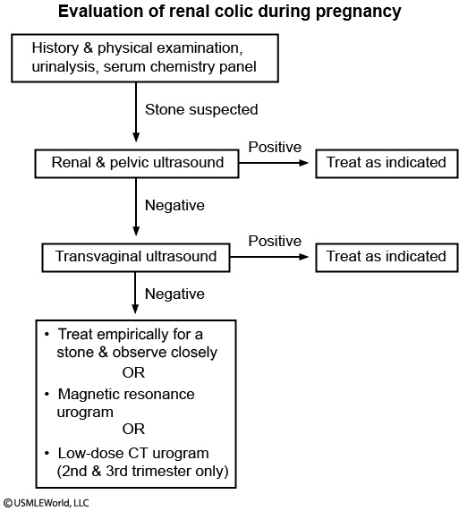
To avoid fetal radiation exposure, diagnosis of nephrolithiasis during pregnancy is via renal and pelvic ultrasound (US) (Choice B). Ultrasonography usually does not visualize a stone; however, US findings of hydronephrosis and hydroureter are consistent with ureteral obstruction due to nephrolithiasis. Most stones pass spontaneously; therefore, management of nephrolithiasis in pregnancy is generally supportive with pain control as needed. Nephrolithiasis that is complicated by persistent obstruction, intractable pain, or urinary tract infection may require surgical management.