myocarditis
- related: Cardiology
- tags: #cardiology
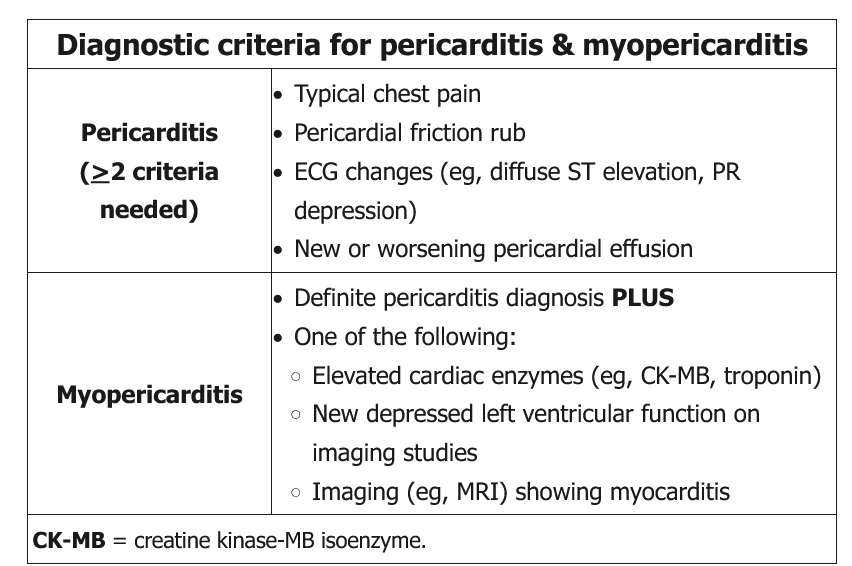
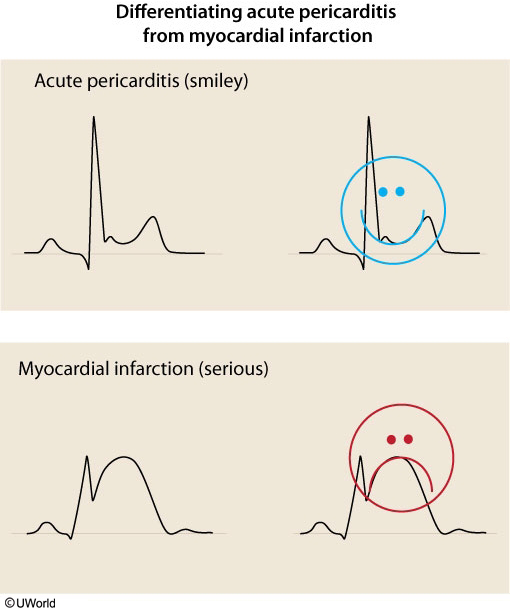
This patient's chest pain, characteristic ECG findings of diffuse ST elevations, and mildly elevated troponin are likely due to viral myopericarditis, defined as acute pericarditis with myocardial involvement noted with either elevated cardiac enzymes, myocarditis on cardiac MRI, or newly depressed left ventricular function.
Pericarditis and myopericarditis share the same etiologies, which, in developed countries, are largely viral or idiopathic. Other causes include bacterial and fungal infections, autoimmune disease (particularly lupus), neoplasms, end-stage renal disease, and postcardiac injury (Dressler syndrome). Presenting manifestations may include pleuritic chest pain (often after viral infection), heart failure, or arrhythmias. Cardiac MRI and, in rare cases, endomyocardial biopsy may help with diagnosis.
Treatment for uncomplicated myopericarditis (normal ejection fraction, no arrhythmias) mirrors that of pericarditis:
- Nonsteroidal anti-inflammatory drug (NSAID) therapy (eg, aspirin, indomethacin, ibuprofen) is the standard of care to control pain and reduce inflammation and should be started on all patients without contraindications (Choices A and D). In patients with postmyocardial infarction pericarditis, aspirin is the NSAID of choice as other medications may inhibit cardiac scar formation.
- Colchicine is recommended in conjunction with NSAIDs to improve symptoms and decrease the rate of recurrence (Choice B).
This patient should receive NSAIDs and colchicine as he has contraindications to neither. By contrast, glucocorticoids, including prednisone, should be avoided as they are associated with a higher rate of recurrence and are only indicated in refractory pericarditis despite NSAID therapy, in patients in whom NSAIDs are contraindicated, or for treatment of a specific underlying cause of pericarditis (eg, autoimmune disease, connective tissue disorders, end-stage renal disease). If an underlying cause is determined, appropriate therapy (eg, antibiotics, antifungals, immunosuppressives) should be initiated.
(Choice C) Intravenous immune globulin may maintain long-term remission in corticosteroid-dependent patients with recurrent episodes of pericarditis.