metabolic alkalosis
- related: Nephrology
- tags: #nephrology
Metabolic Alkalosis
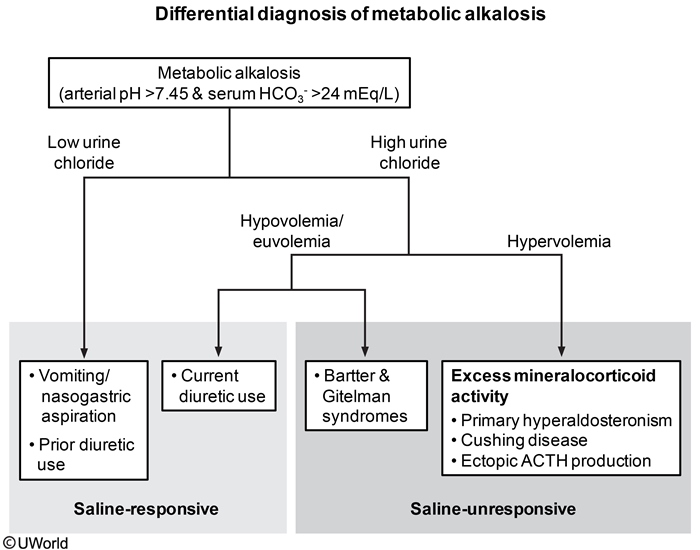
This patient's presentation is consistent with metabolic alkalosis, defined as arterial pH >7.45 and serum bicarbonate level >24 mEq/L. Metabolic alkalosis can be further classified as saline-responsive and saline-unresponsive. It can also be classified according to low (<20 mEq/L) or higher levels of urinary chloride. Saline-unresponsive metabolic alkalosis typically presents with a higher level of urinary chloride (>20 mEq/L). Patients can have expanded extracellular fluid (ECF) with hypervolemia (eg, primary hyperaldosteronism, Cushing syndrome, excessive black licorice ingestion) or appear hypo/euvolemic (eg, Bartter syndrome, Gitelman syndrome). These conditions require treatment of the underlying disorder; the metabolic alkalosis is not corrected by saline infusion alone.
Saline-responsive metabolic alkalosis is commonly due to loss of gastric secretions (eg, self-induced or spontaneous vomiting, nasogastric suctioning) that results in ECF loss. Patients typically develop volume depletion (eg, hypotension, orthostasis) and low serum Cl- due to chloride loss in the gastric secretions. The ECF loss leads to increased renal mineralocorticoid levels, increased renal sodium and chloride reabsorption, and increased urinary H+ and K+ excretion. The end result is decreased urine chloride, hypokalemia, and metabolic alkalosis. Prior use of thiazide or loop diuretics will also lower urine chloride, but current diuretic use increases urine chloride. Low serum Cl- also impairs renal HCO3- excretion and further worsens the alkalosis. Saline-responsive metabolic alkalosis usually corrects with isotonic saline infusion alone and restores both ECF volume and low serum Cl-.