mechanical heart valve anticoagulation
- related: Valvular Diseases, Cardiology
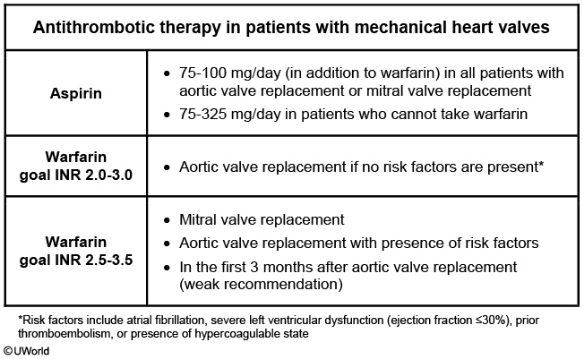
The risk of systemic thromboembolism (eg, stroke) is approximately 4% per patient per year in those with mechanical prosthetic valves with no anticoagulation, compared to about 2% in patients treated with aspirin, and <1% in patients treated with warfarin. Patients with mechanical mitral valves have twice the risk compared to those with aortic valve prostheses. Therefore, long-term treatment with aspirin and warfarin is recommended for all patients with mechanical aortic or mitral valve replacement to reduce the rates of systemic thromboembolism.
Current guidelines on the target International Normalized Ratio (INR) vary with the valve position (aortic vs mitral), type of mechanical valve, and associated comorbid conditions. In patients with mechanical aortic valve and no other risk factors (eg, atrial fibrillation, severe left ventricular dysfunction [ejection fraction <30%], prior thromboembolism, presence of hypercoagulable state), guidelines recommend long-term treatment with aspirin and warfarin to achieve a goal INR of 2.0-3.0.