management of renal cysts
- related: Nephrology
- tags: #nephrology
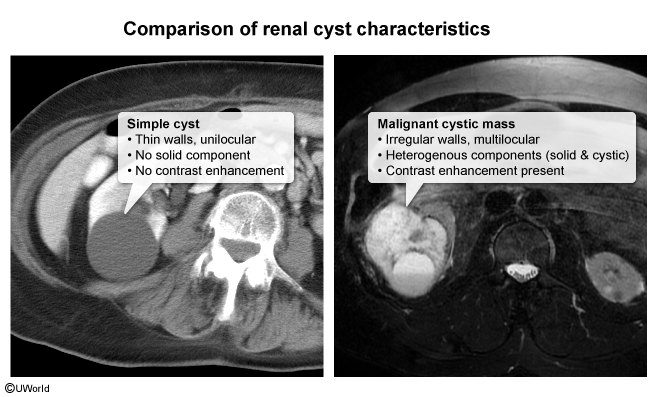
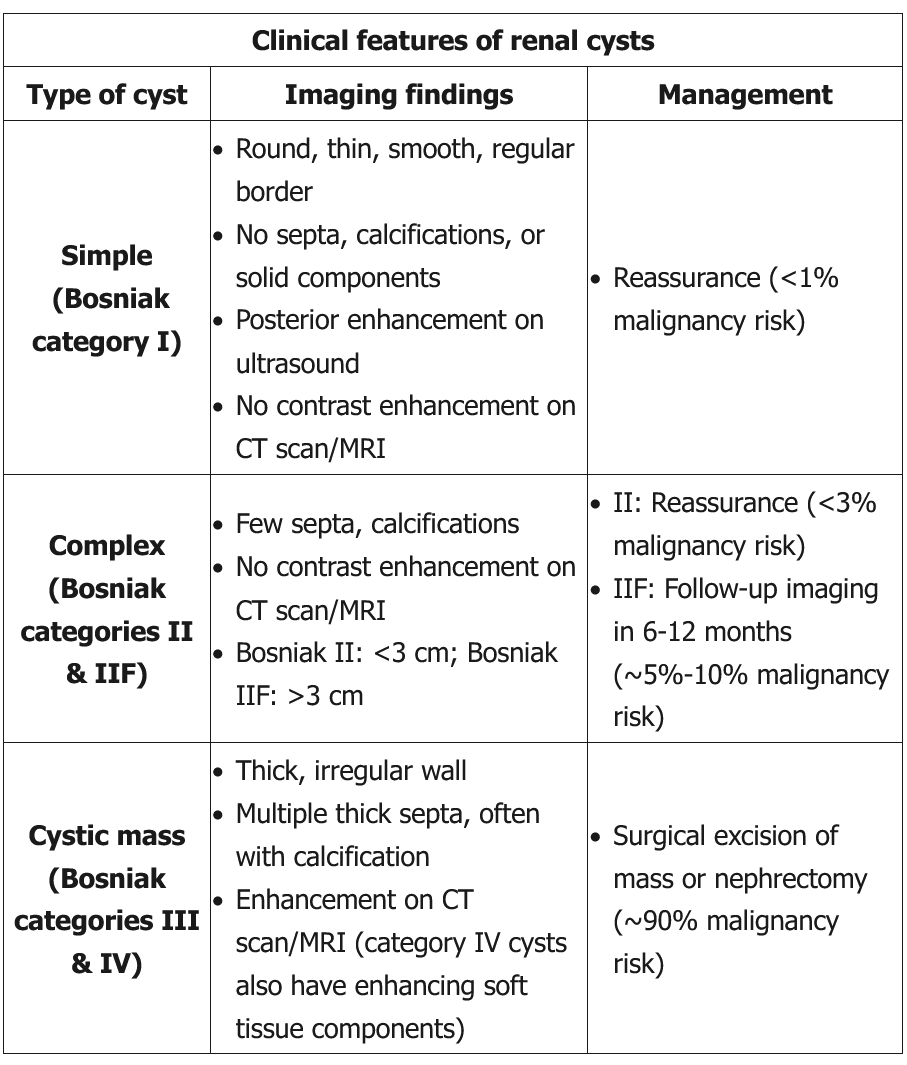
Renal cysts are classified as simple or complex based on imaging characteristics. Most (60%-70%) are simple cysts (Bosniak category I), occurring more commonly at age >50. These cysts are typically asymptomatic and do not cause renal damage or hypertension; they can be solitary/multiple or unilateral/bilateral. As seen in this patient, a simple cyst can be diagnosed using ultrasound alone when all of the following features are present:
-
A round mass with thin, smooth walls
-
Clear (anechoic) fluid
-
Posterior wall enhancement (a technical artifact seen on ultrasound studies that indicates ultrasound wave transmission beyond the cyst; it does not equate with contrast enhancement on CT scan/MRI)
For a simple cyst, CT scan/MRI is not required for diagnosis but would reveal no contrast enhancement (ie, avascular lesion). Because simple cysts have a very low malignancy risk (<1%), patients can be reassured without the need for follow-up imaging unless complications (eg, infection, hemorrhage, pain) are suspected.
Complex cysts (Bosniak categories II and IIF) have more septations, calcifications, or changes in wall size. CT scan/MRI with contrast reveals no measurable enhancement. Complex cysts with certain features (see Bosniak IIF in table) have a higher risk (~5%-10%) of malignancy and require follow-up imaging in 6-12 months (Choice E). Cystic masses (Bosniak categories III and IV) have a thick, irregular wall with multiple thick septa that are often calcified. Lesions usually enhance on CT scan/MRI, and category IV lesions have enhancement in soft tissue components adjacent to the wall or septum. Cystic masses are usually surgically resected given the higher risk (~90%) of malignancy. Complex cysts with measurable enhancement are treated as cystic masses. Some clinicians adopt a more conservative approach for Bosniak category III cysts (eg, needle biopsy, close monitoring with repeat imaging).
CT scan of the abdomen is usually reserved for lesions with indeterminate ultrasound findings. CT scan with intravenous contrast can assess for contrast enhancement (increased density >10-15 Hounsfield units) in the cyst, which increases the risk for malignancy.