male hypogonadism
- related: Endocrine
This patient has symptoms (ie, decreased libido, possible early testicular atrophy) that warrant testing for hypogonadism. His loss of early-morning (nonsexual) erections suggests an organic (rather than psychogenic) cause of erectile dysfunction. Hypogonadism is common in men with obesity and/or diabetes/prediabetes, likely due to dysfunction of the hypothalamic pituitary axis.
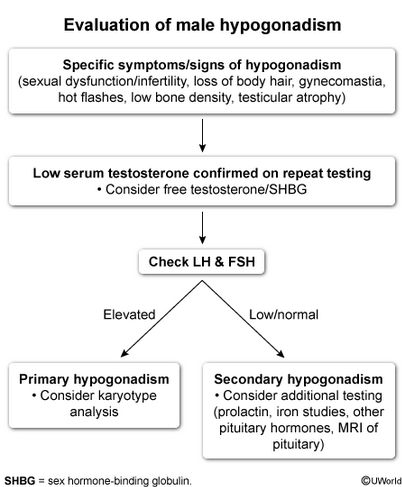
Other specific features that should prompt evaluation for androgen deficiency include loss of body hair, gynecomastia, hot flashes, and an unexplained decrease in bone density. In contrast, nonspecific symptoms (eg, fatigue, weakness, weight changes) alone do not warrant testing in most cases. The initial step in evaluation of male hypogonadism is a morning serum total testosterone level. However, testosterone shows significant variability, and low levels should be confirmed on repeat testing.
(Choice A) Although obesity and diabetes are associated with true hypogonadism, these conditions are also associated with decreased levels of sex hormone–binding globulin, leading to spuriously low total testosterone levels. If the initial total testosterone level is low, measurement of free testosterone levels should be considered to confirm true hypogonadism in patients with these conditions; however, testing is not recommended in the initial workup of hypogonadism because it requires specialized assays that can be expensive and inaccurate and are not always readily available.
(Choices B and C) If testosterone is low, serum FSH and LH levels can distinguish primary (elevated LH and FSH) from secondary (low/normal FSH and LH) hypogonadism. MRI of the pituitary should be considered in patients with secondary hypogonadism and for those with severe hypogonadism (eg, testosterone <150 ng/mL), deficiencies of additional pituitary hormones (eg, TSH, growth hormone), hyperprolactinemia, or mass effect symptoms (eg, visual field defects).
(Choice D) Nocturnal penile tumescence can be useful in differentiating psychogenic (normal) and organic (reduced tumescence) causes of erectile dysfunction. However, it is not commonly used in clinical practice, and the decreased morning erections in this patient suggest an organic cause.
- testosterone has diurnal varriation
- obtain testosterone at 8 am
- repeat morning measurement if low
- If low, LH and FSH to determine origin
- primary: elevated LH/FSH
- secondary: low or inappropriately normal LH/FSH
- initiate exogenous testosterone therapy
- check levels at 3 and 6 months after, then annually
- goal mid-normal range