Kawasaki
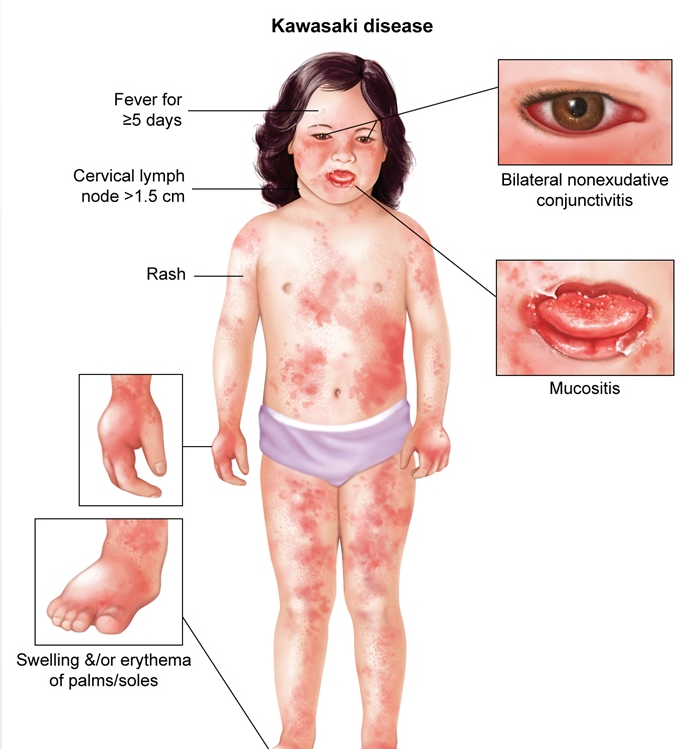
This boy age <5 has had fever for 5 days as well as the following symptoms:
- Rash (inguinal folds, perineum, trunk)
- Nonexudative conjunctivitis
- Mucositis (erythematous lips, tongue ["strawberry tongue"], oral mucosa)
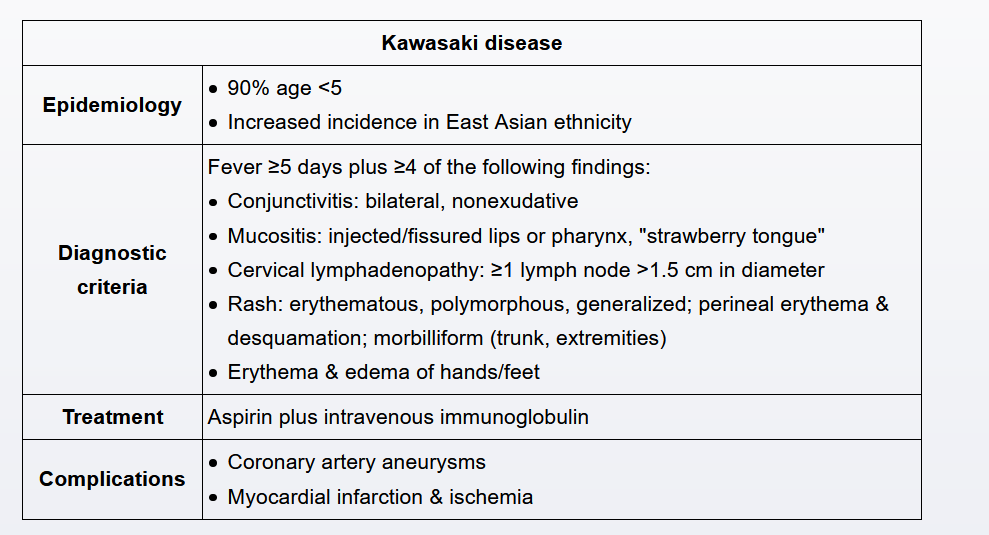
He therefore meets 3 of the 5 diagnostic criteria of Kawasaki disease (KD), a febrile vasculitis of unknown etiology. An additional criterion (cervical lymphadenopathy or extremity erythema/edema) is required for diagnosis. However, KD symptoms often do not manifest simultaneously; therefore, when <3 diagnostic criteria are met in a child with >5 days of fever, C-reactive protein or erythrocyte sedimentation rate (inflammatory markers that are elevated in KD) should be ordered, with daily follow-up scheduled to assess for new symptoms.
KD can present a diagnostic challenge because viral illnesses can cause fever >5 days and similar features (eg, rash, conjunctivitis, oropharyngeal erythema). However, failure to treat KD in a timely manner significantly increases the risk of serious sequelae (eg, coronary artery aneurysms), with substantial risk after the 10th day of illness. Therefore, unless a definite alternate diagnosis has been established, waiting 3-4 days without performing laboratory studies or reexamination is inappropriate
Besides fever, the patient now fulfills 4 diagnostic criteria for Kawasaki disease (KD): rash, conjunctivitis, mucositis, and extremity edema/erythema. Therefore, a definitive diagnosis can be made. (The fifth diagnostic criterion, lymphadenopathy, is the least frequently observed.)
The first step in treatment is administration of intravenous immunoglobulin (IVIg). It is administered in conjunction with aspirin, which reduces systemic inflammation. Although its exact mechanism of action in KD is unknown, the use of IVIg greatly improves morbidity and mortality and significantly decreases the risk of cardiac sequelae.
All children diagnosed with Kawasaki disease (KD) should have an echocardiogram performed at baseline. Although coronary artery aneurysms usually develop after the 10th day of fever and are often not evident during acute illness, some degree of coronary artery dilation and myocardial dysfunction may be present at diagnosis. Aneurysms may later develop even in patients who receive appropriate treatment, so follow-up studies are indicated at 2 and 6 weeks after treatment, even if the initial study is normal. Due to the high risk of sequelae in patients with KD, it would be inappropriate to omit echocardiography even in the absence of any cardiac complaints (eg, chest pain, difficulty breathing)
The patient has been treated with intravenous immunoglobulin (IVIg), which is composed of pooled antibodies. These antibodies interfere with the body's normal immune response to live vaccines. Because of this, patients should defer live vaccines for 11 months after receiving IVIg.
The vaccines typically administered at age 4 include live vaccinations (second dose of measles-mumps-rubella and varicella), so they should be postponed in this 39-month-old patient until the appropriate amount of time has elapsed.