hypogonadotrophic hypogonadism
- related: Endocrine
- tags: #endocrine
In Diabetes
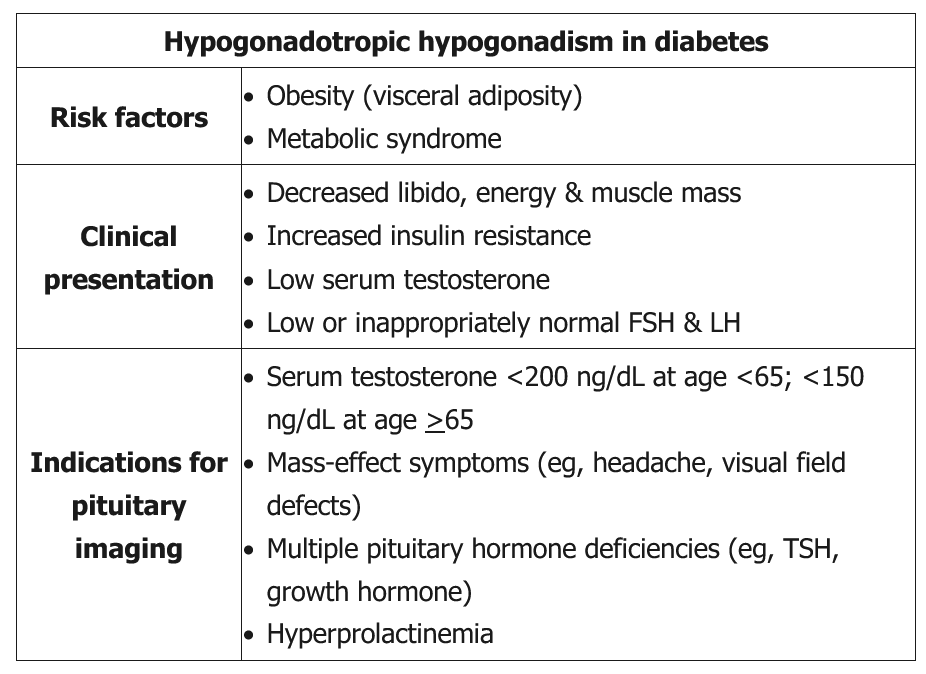
This patient has hypogonadal symptoms with a low serum testosterone level and low/inappropriately normal FSH and LH levels. This is consistent with hypogonadotropic (central) hypogonadism. Hypogonadism is common in men with type 2 diabetes, especially those age >65 or with concurrent obesity. For this reason, some experts have recommended regular screening with serum testosterone in patients with diabetes.
Older (ie, age >65) obese men with type 2 diabetes typically have low-normal to mildly low serum testosterone levels (200-300 ng/dL) due to decreased gonadotropin release from the anterior pituitary (likely obesity mediated), as well as physiologic changes in testosterone metabolism (eg, decreased sex hormone-binding globulin). These patients do not need pituitary imaging. However, younger men with more pronounced declines in serum testosterone (as in this patient) and/or abnormalities in additional pituitary hormones (eg, central hypothyroidism) are more likely to have sellar masses or other structural disruptions of the hypothalamic-pituitary axis (eg, infiltrative disease). These patients should have pituitary imaging, preferably with MRI.