hypertension with primary hyperaldosteronism
- related: Nephrology, Cardiology
- tags: #nephrology
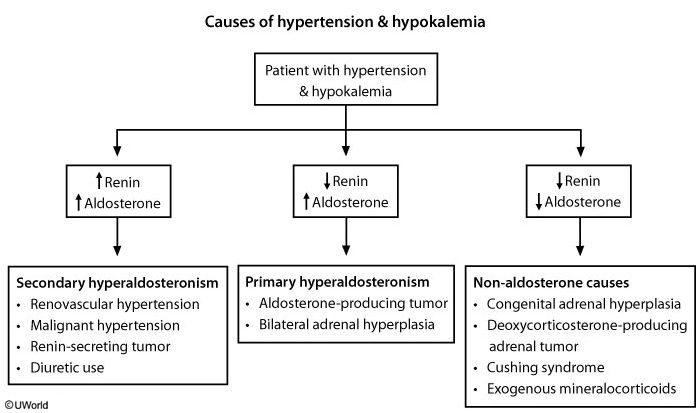
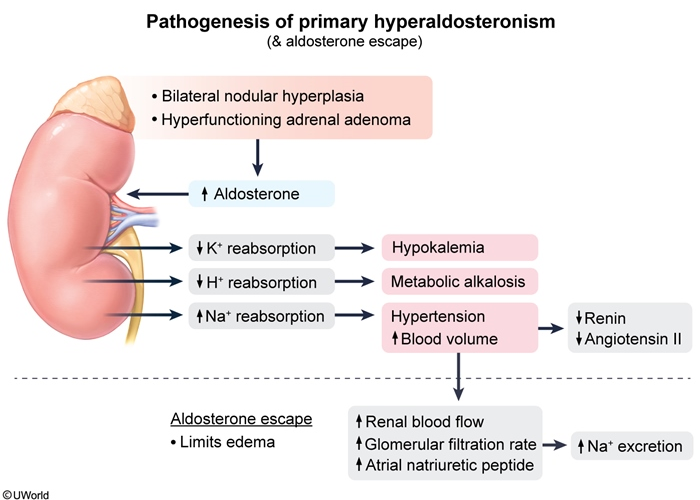
Primary hyperaldosteronism (PH) is characterized by hypertension associated with hypokalemia and metabolic alkalosis. Some patients may not have spontaneous hypokalemia but rapidly develop hypokalemia if given diuretics. Despite increased renal reabsorption of sodium, edema and hypernatremia are usually minimal or absent due to aldosterone escape.
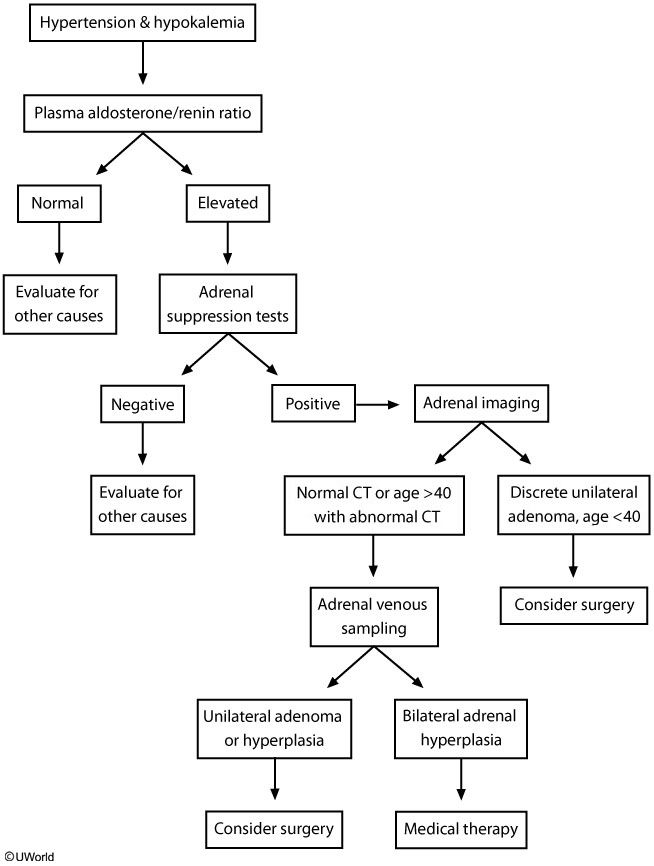
The initial evaluation for PH should include a morning plasma aldosterone concentration (PAC) to plasma renin activity (PRA) ratio. A PAC/PRA ratio >20 with plasma aldosterone >15 ng/dL suggests PH. The diagnosis is most often confirmed with an aldosterone suppression test (either an oral sodium load test or a saline infusion test); persistent aldosterone production despite an oral or intravenous sodium load confirms PH. However, for patients with spontaneous hypokalemia, undetectable PRA, and PAC >30 ng/dL (as seen in this patient), confirmatory adrenal suppression testing may be omitted as the findings are unlikely to be from any other cause.
Once PH is confirmed, adrenal imaging (usually with CT scan) should be obtained to differentiate bilateral adrenal hyperplasia (50%-60%) from aldosterone-producing adrenal adenoma (40%-50%). However, CT has low sensitivity for small tumors; therefore, if CT does not reveal a discrete unilateral mass (as with this patient), adrenal venous sampling should be obtained to differentiate between hyperplasia and adenoma.
Renal CT angiogram is used to diagnose renovascular hypertension due to renal artery stenosis or fibromuscular dysplasia. However, renovascular hypertension is associated with secondary hyperaldosteronism (elevated renin and aldosterone levels), not primary.