hydatidiform mole
- related: OBGYN
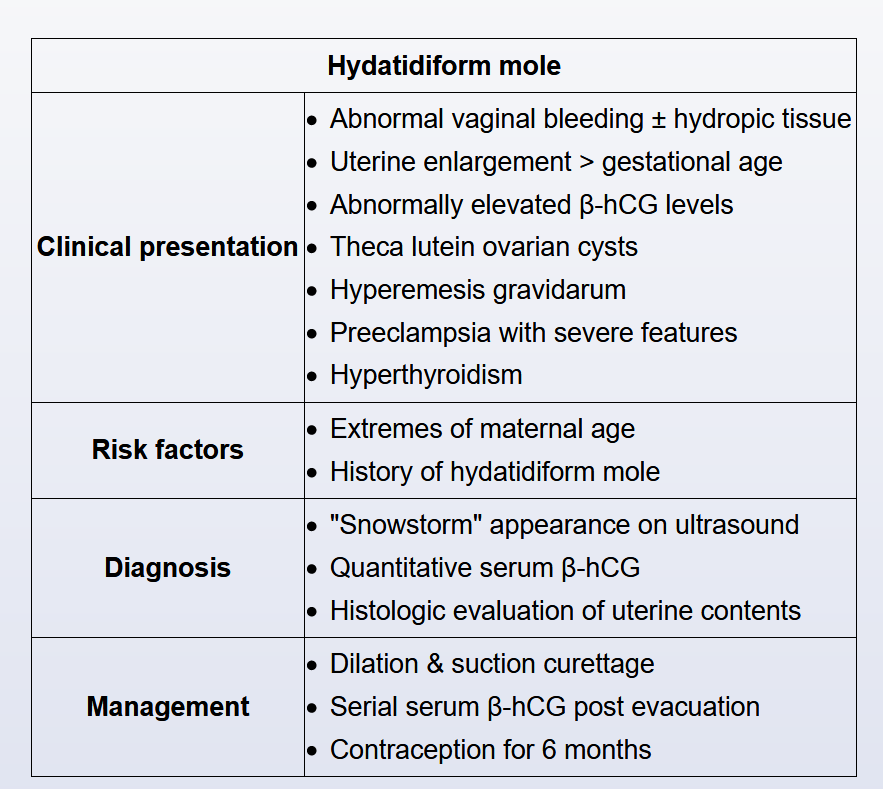
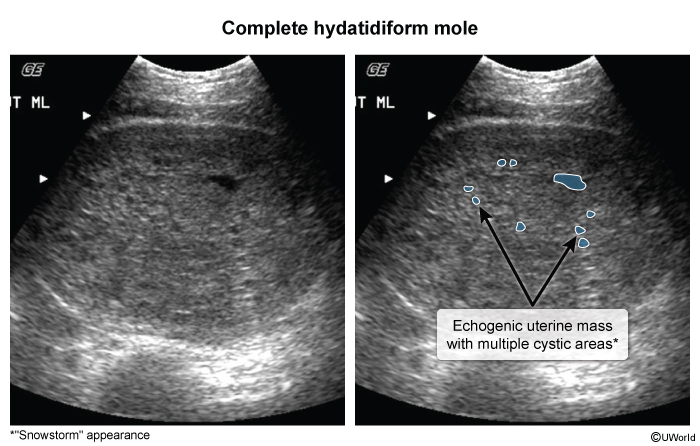
This patient's secondary amenorrhea, markedly enlarged uterus (infraumbilical mass), and hyperthyroidism are consistent with a hydatidiform mole, an abnormal gestation that results from the fertilization of an empty ovum. Additional clinical features can include hyperemesis gravidarum, abnormal vaginal bleeding, and bilateral enlarged ovaries (eg, theca lutein cysts). Risk factors for hydatidiform mole include extreme maternal age (eg, <15, >35) and a history of hydatidiform mole.
Hydatidiform moles are characterized by markedly elevated β-hCG levels (>100,000 mIU/mL) that occur as a result of trophoblastic tissue hypertrophy. The α subunit of hCG is structurally similar to thyroid-stimulating hormone and can stimulate the thyroid gland to produce T3 and T4. Patients who have a hydatidiform mole and present at later gestational ages (eg, second trimester), when hCG levels have been markedly elevated for a prolonged time, can have symptoms of hyperthyroidism (eg, warm, dry skin; anxiety; weight loss; hypertension; tachycardia; tremor).
Treatment of hydatiform mole is with suction curettage. Because surgery can instigate thyroid storm in patients with hydatidiform moles that are complicated by hyperthyroidism, beta adrenergic blockers are often administered preoperatively.