esophageal perforation
- related: GI
- tags: #GI
This patient's presentation suggests spontaneous esophageal rupture (SER). SER (Boerhaave syndrome) is usually due to prolonged nausea and vomiting causing an acute rise of intraesophageal pressure combined with negative intrathoracic pressure. This leads to a transmural esophageal tear and acute barotrauma with esophageal air/fluid leaking into surrounding areas (eg, mediastinum, pleura). Although it is a rare diagnosis, SER has a 20% mortality rate, usually due to infectious complications (eg, empyema, mediastinitis, septic shock).
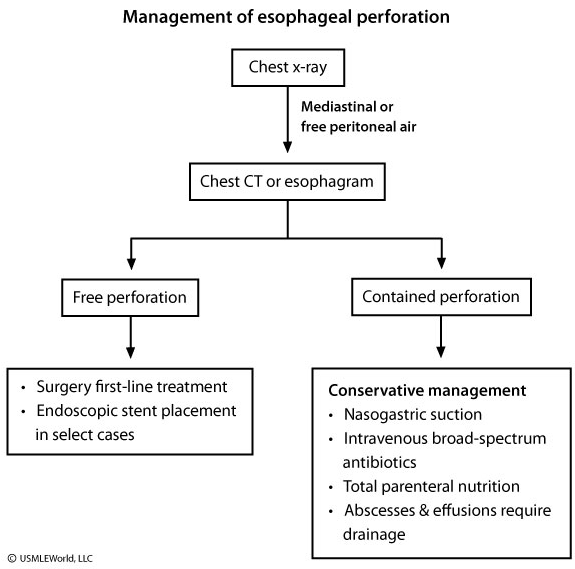
Patients usually present with vomiting/retching and chest/upper abdominal pain with rapid progression to odynophagia, fever, dyspnea, and septic shock. Physical examination may show subcutaneous emphysema but is not a sensitive finding. Chest x-ray may reveal pneumomediastinum or pleural effusions. Pleural fluid analysis is typically exudative with low pH and very high amylase (> 2500 IU). Computed tomography or contrast esophagography with Gastrografin is preferred for confirming the diagnosis.
Esophagogastroduodenoscopy (EGD) with insufflation of air can extend the perforation and introduce air into the mediastinum. However, when done under a controlled setting in the operating room, EGD may be useful for select patients to directly visualize the perforation and plan treatment.