elevated PSA management
- related: Urology, prostate cancer
- tags: #note
This patient’s presentation of irritative and obstructive lower urinary tract symptoms, normal urinalysis, large prostate without a focal lesion, and prostate-specific antigen (PSA) > 10 ng/mL is consistent with a prostatic disorder. PSA values have a log-linear relationship with prostate volume. However, elevated PSA has a lower specificity for prostatic cancer in men with obstructive symptoms than asymptomatic men.
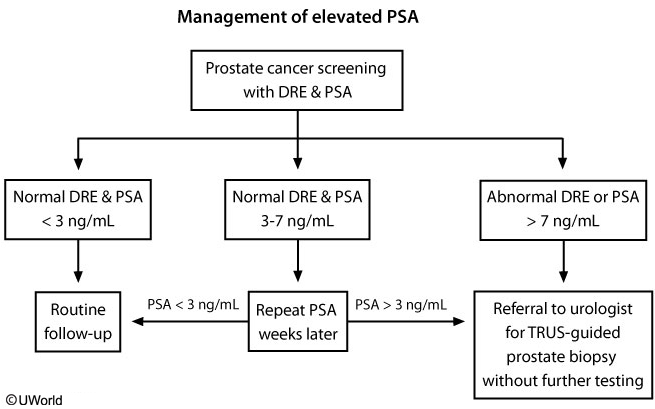
Prostate cancer screening is an individualized decision, and clinicians should first discuss the risks and benefits. If the patient prefers screening, most clinicians perform a digital rectal examination (DRE) and test serum PSA. Patients with normal DRE and PSA < 3 ng/mL may be followed routinely. Men with PSA > 7 ng/mL or abnormal DRE should be referred to a urologist for possible biopsy. Patients with PSA of 3-7 ng/mL should be retested in a few weeks and referred to a urologist if PSA remains > 3 ng/mL (Choice C).
Although the most common cause of elevated PSA is benign prostatic hyperplasia (BPH), the positive predictive value of a PSA > 10 for prostate cancer is 15%-40%. Thus, this patient should be referred to a urologist.
(Choices A and B) 5-alpha-reductase inhibitors and alpha-1-adrenergic blockers may relieve moderate to severe BPH symptoms. Treatment usually requires several weeks for optimal effect. However, this patient’s mild BPH symptoms and elevated PSA require further investigation.
(Choice E) A renal ultrasound would not be helpful with a normal serum creatinine. However, transrectal prostatic ultrasound can help guide prostate biopsy in selected cases.