diabetes management
- related: Endocrine
- tags: #note
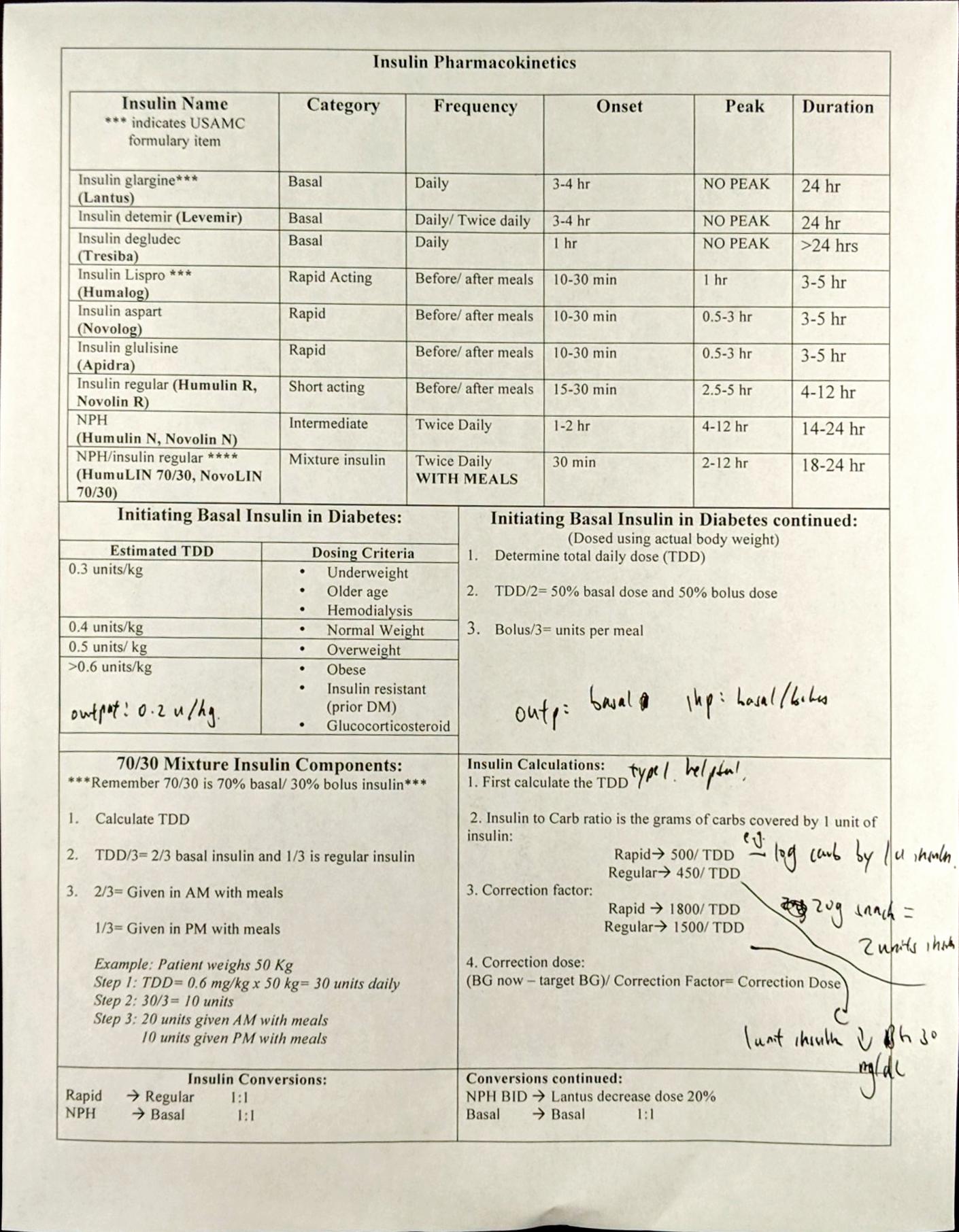
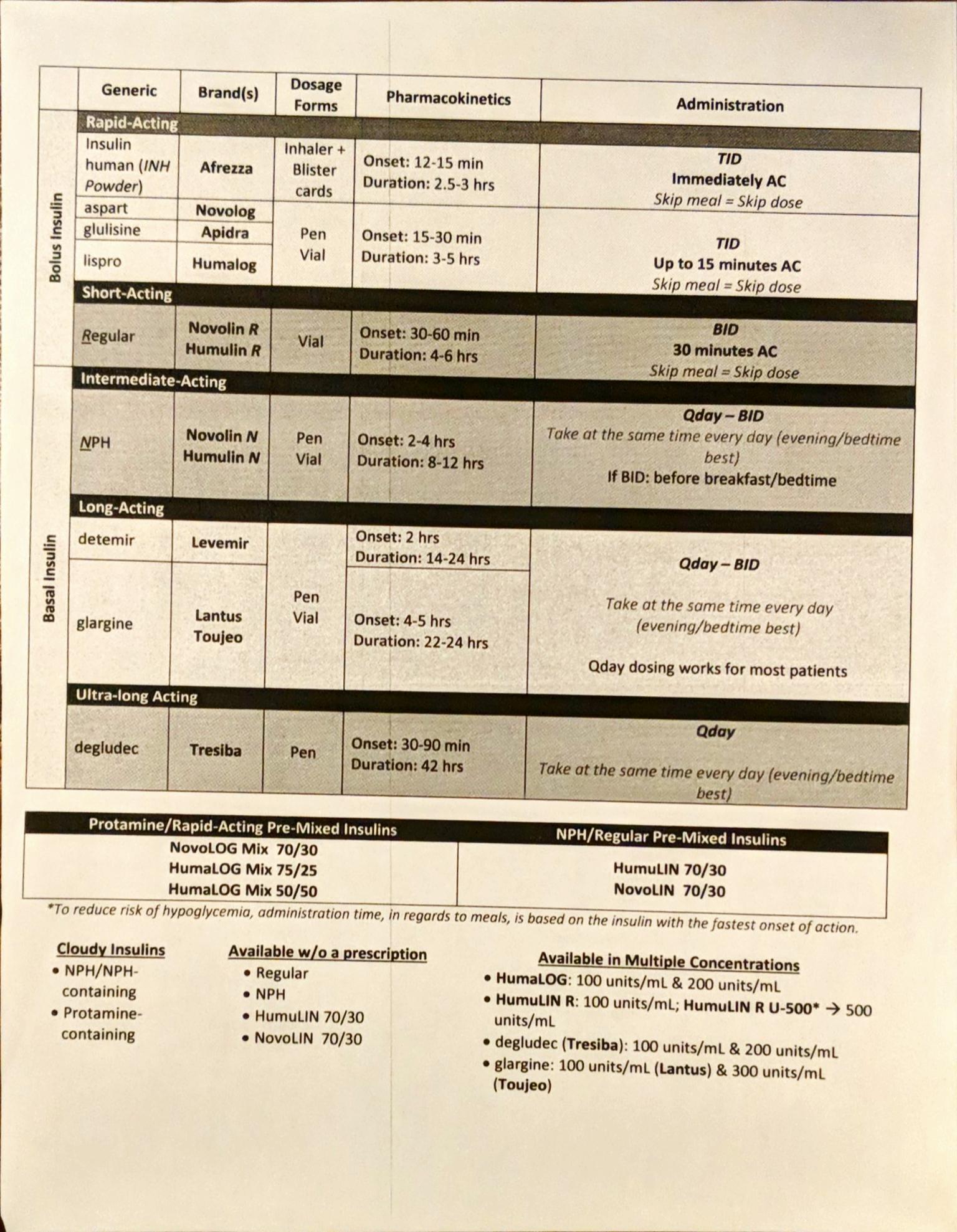
Types of insulin
- short acting: regular; onset 30 min - 1 hour
- rapid acting: NPH, lispro; onset 15 - 30 min
- Lantus (glargine): given sometimes once and sometimes twice a day.
- Levemir (detemir): does not last 24 hours, only lasts 12
- NPH: 12 hours, give 2x/day
- Humulin-R: 6 hours, give with meals, only use if can't afford others
- U-500: 500 units of concentrated insulin, use when using more than 300 u/day. Use like humulin R but like a basal. 60% in morening, 40% at night or 40-30-30
- 70/30: mixed
- 70% basal (NPH), 30% short acting
- start at 0.5/u/kg/day
- dosed BID
- only use if struggling with injections
- You can convert to long acting by multiplying 70% of total 70/30
- SSI: check glucose, then give insulin based on sugar and food given
Weight Based TDD
- Type 1: 0.2-0.4
- Type 2: 0.5-1.0
Outpatient Management
DM2
Goal:
- 2 hours after meal (post prandial): 100-180
- Fasting (FBG): 90-130
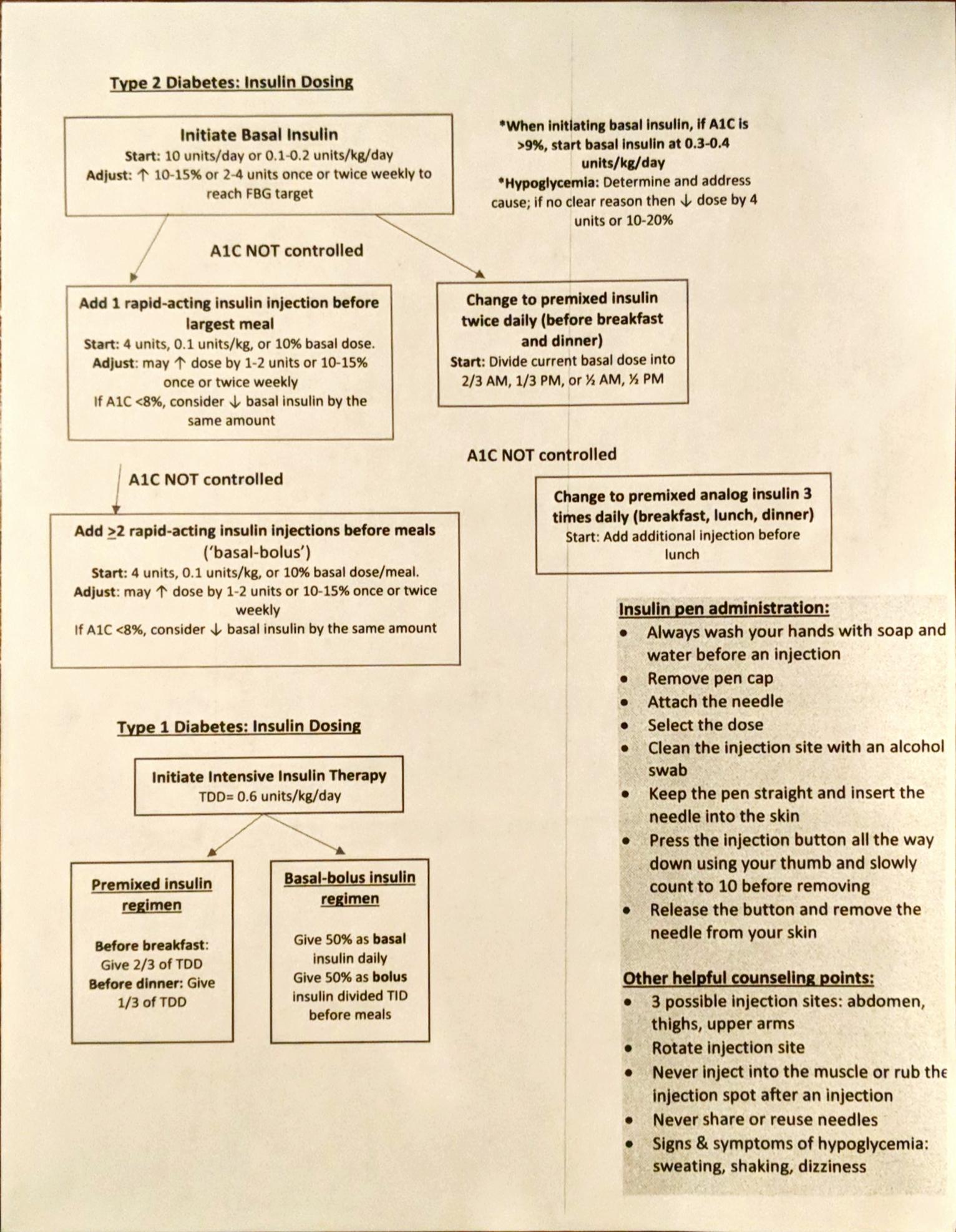
Start with metformin, then go to basal insulin (long acting), then add meal time insulin (short acting)
- start metformin and add oral agents
- start basal insulin if using 3 or more agents or if A1C > 10%. Target FBG
- once fasting is under controlled, recheck A1C in 3 months
- A1C high: start meal time insulin with largest meal of day, then go up to 3x/day if needed
Meal time insulin:
- 2 ways of calculating meal time:
- 10% basal dose = meal time. E.g. 60 units basal insulin, 6 x 3 = 18 units / meal
- 1/2 basal. E.g. 60 units basal, 30 units total / 3 = 10 units / meal
- Can use GLP in place of meal time insulin
A1C to glucose conversion:
- For each 1 point on A1C, BG goes up/down by 30
- 8 = 180
- 9 = 210
DM 1
- start with basal bolus insulin
- weight based dosing 0.2-0.4 u/kg
- spit in 1/2
- 50% basal
- 50% bolus
- count carbs
- give pumps if uncontrolled
Inpatient management
- Goal inpatient and ICU: 140-180
- TF: use regular insulin q6h
- SSI: Use correction factor TDD/1800 = how much glucose drop
- e.g. 100/1800 = 18mg.dl drop
- Insulin pump but not on pump: either use weight based or TDD from pump
Smogyi Effect and Dawn phenomenon
- Smogyi effect: theory of hyperglycemia in early morning due to hypoglycemic events during late evening
- Dawn phenomenon: morning hyperglycemia is due to the decreased levels of endogenous insulin secreted at night. Similar to Smogyi but without hypoglycemic events
charts