depression and anxiety 12 16 note
- related: Psychiatry
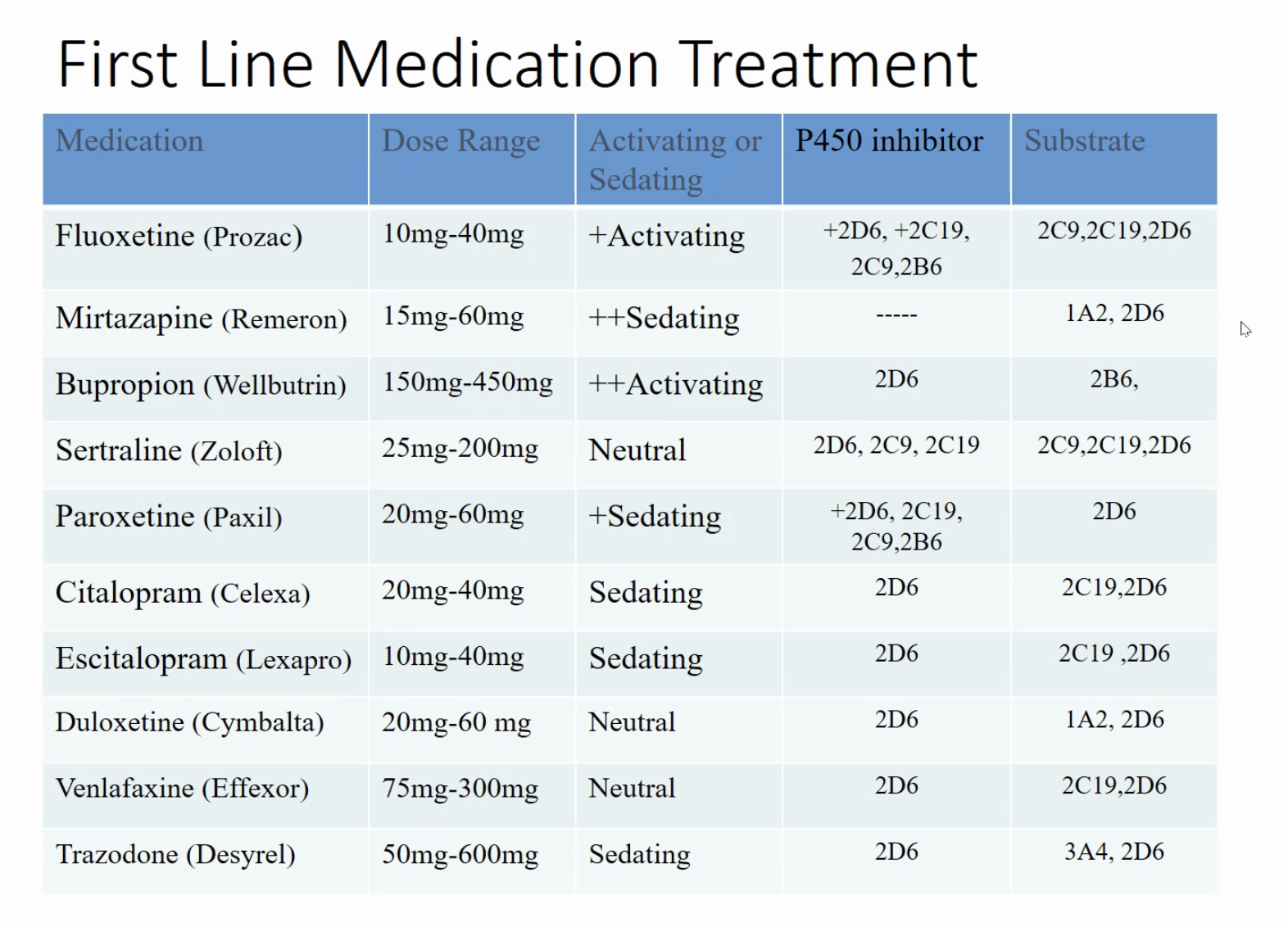
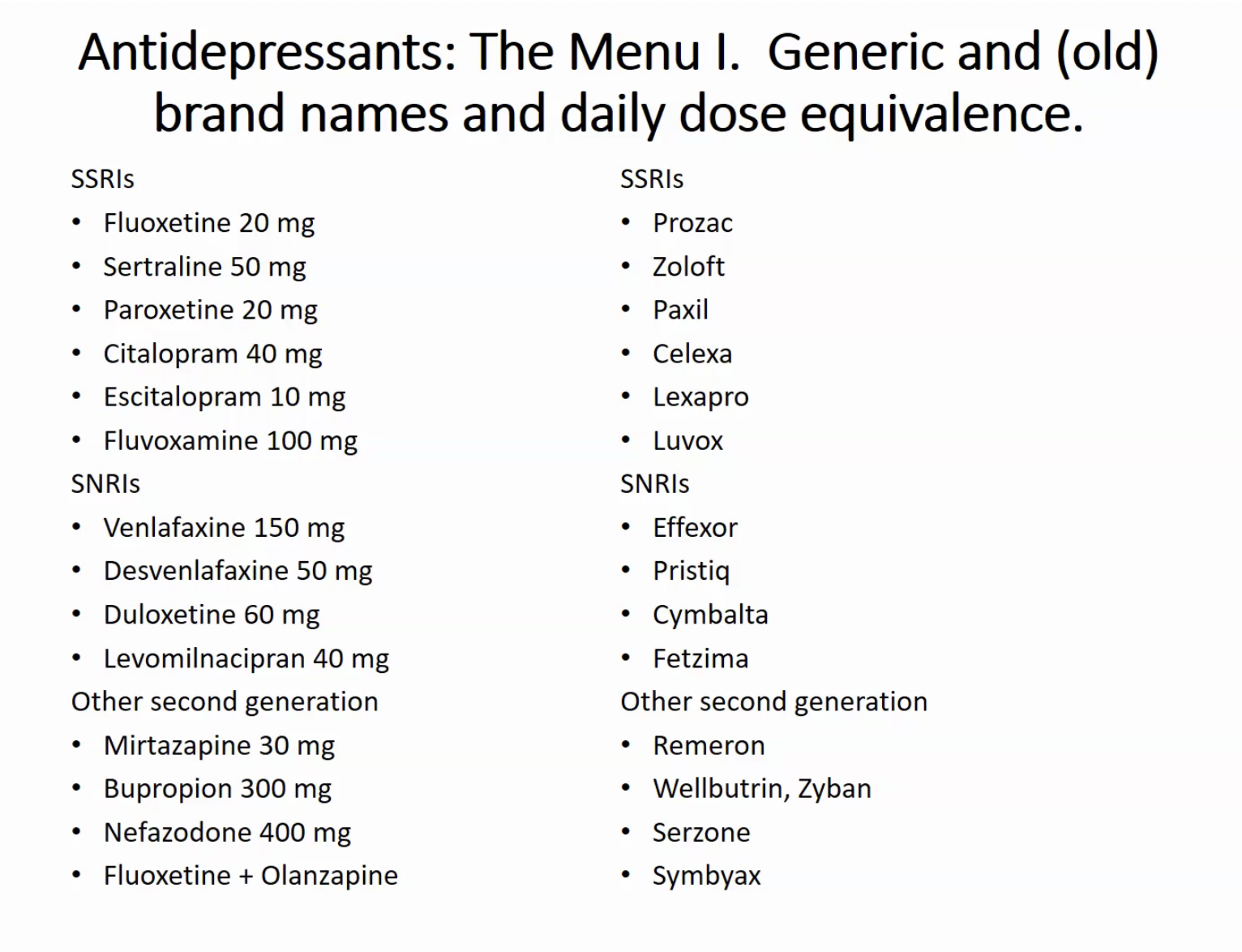
Antidepressant dosing and brand name:
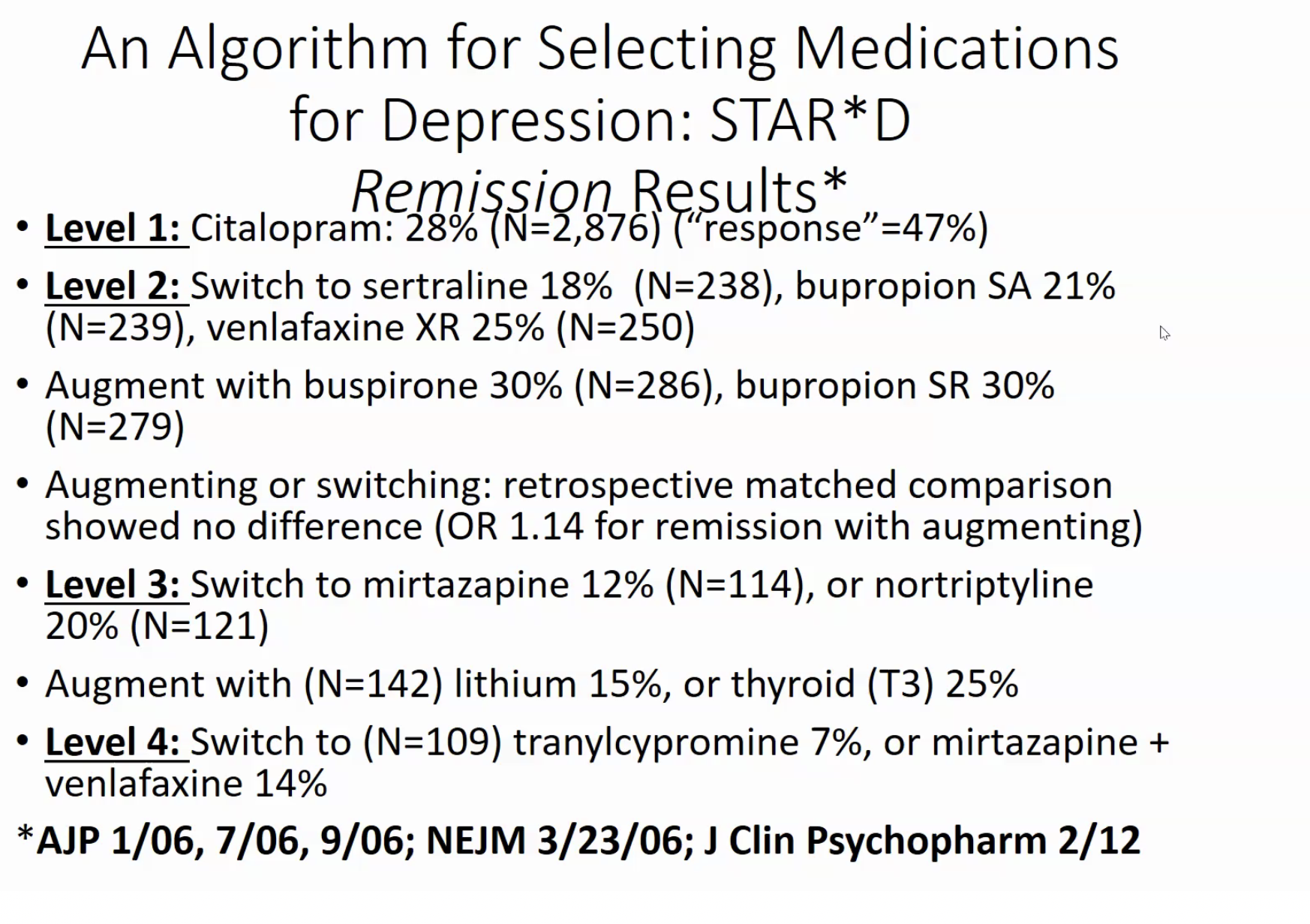
Algorithm for depression treatment:
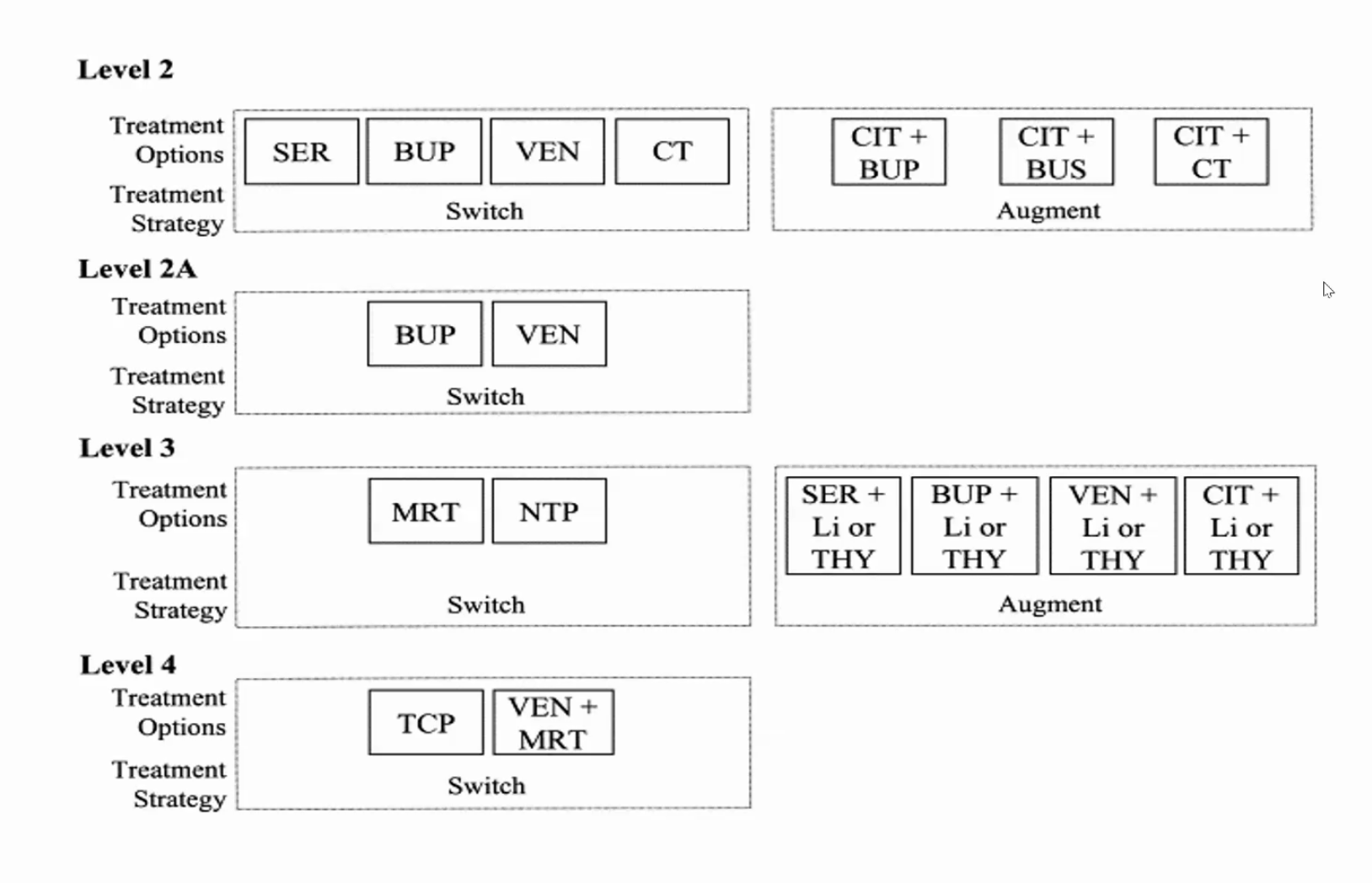
- CT: cognitive behavior therapy
- No huge difference after failing first SSRI
- Paroxetine is most anxiolytic. Citalopram better tolerated and also has anxiolytic. Zoloft also has anxiolytic
Switching antidepressants
- Cross titrate 2 different medications over 2 weeks
Pharmacologic treatment options for patients with treatment-resistant depression include switching to another antidepressant or augmenting with a second agent. This patient has failed to respond to an adequate trial (>6 weeks) of high-dose fluoxetine. Patients with little to no improvement (nonresponders) or unacceptable tolerability generally benefit from switching to another antidepressant rather than augmentation. Discontinuing fluoxetine and starting venlafaxine, a serotonin-norepinephrine reuptake inhibitor, would be the most appropriate next step.
Partial responders, in contrast, can consider augmentation as a first-line option as switching carries a risk of losing the partial therapeutic benefit from the original drug. Augmentation strategies include adding a second-generation antipsychotic, an antidepressant with a different mechanism of action, or occasionally lithium or triiodothyronine.
The second-generation antipsychotic aripiprazole is an effective augmentation strategy for treatment-resistant major depression. However, it is not used as monotherapy.
Side Effects
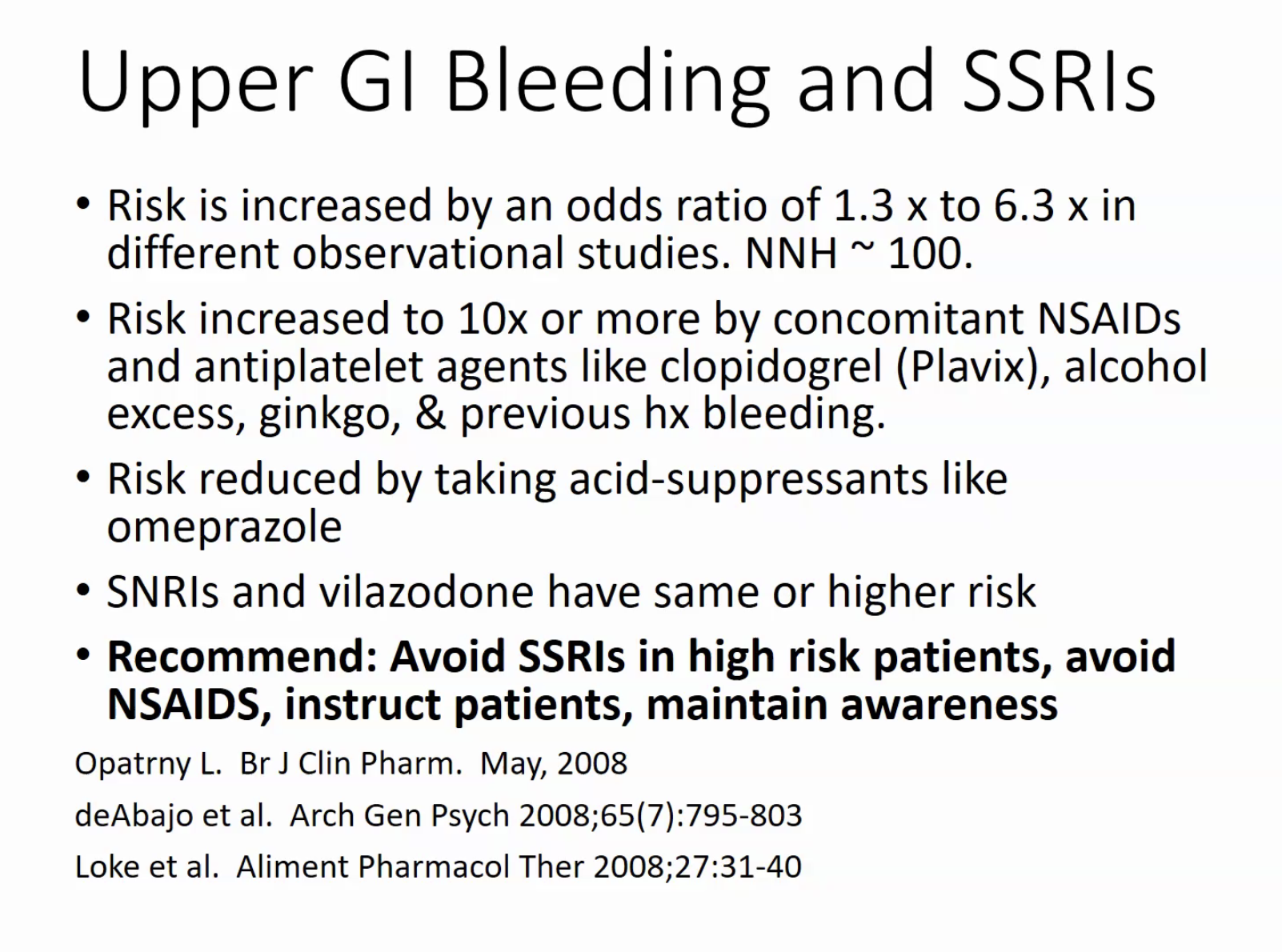
- Increase GI bleed with SSRI
- Citalopram can cause increased QTc, check in elderly
- Paxil: most anticholinergic, bad for elderly
- Prozac: very long acting, can be too activating in elderly
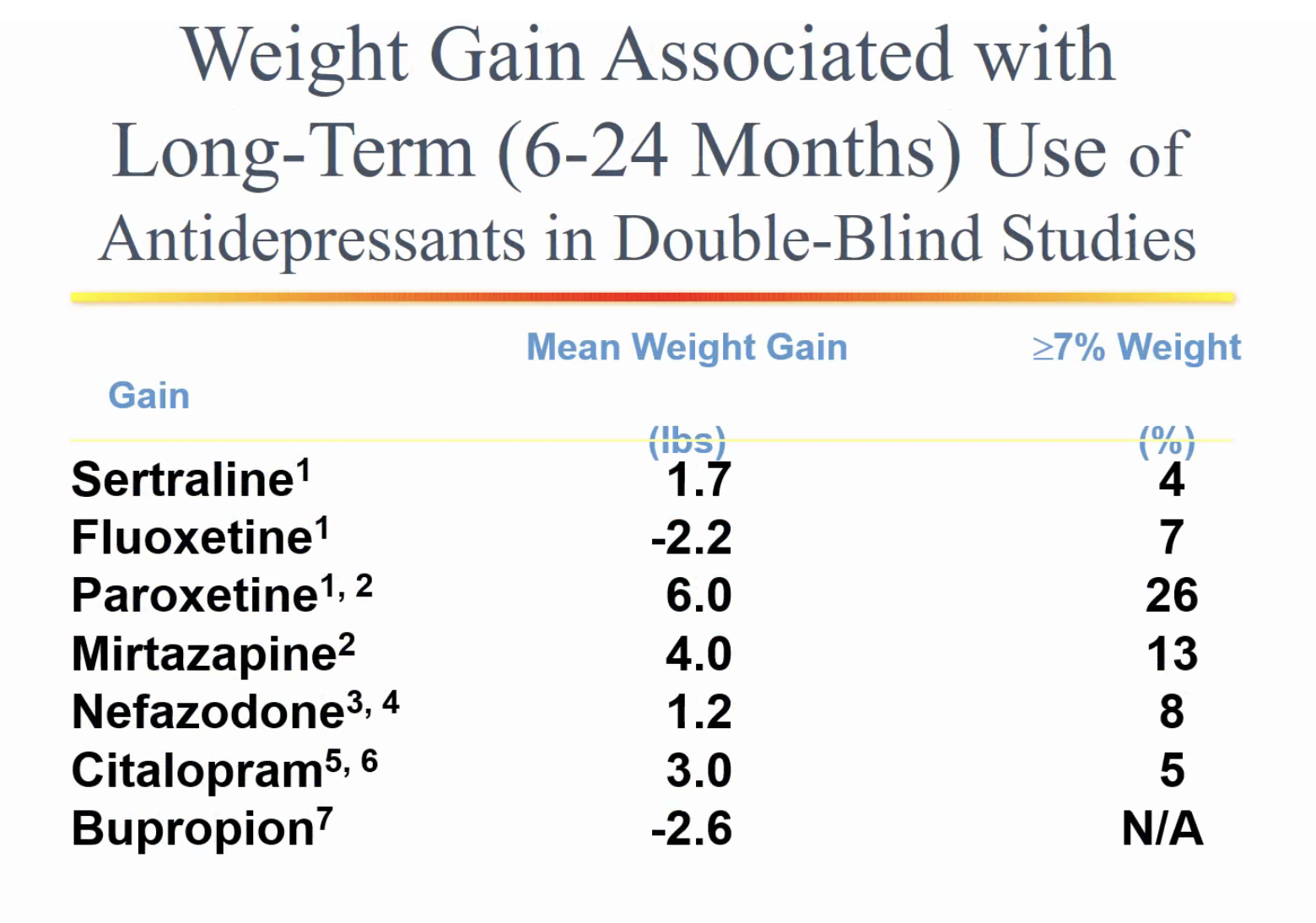
- weight gain:
Sleep
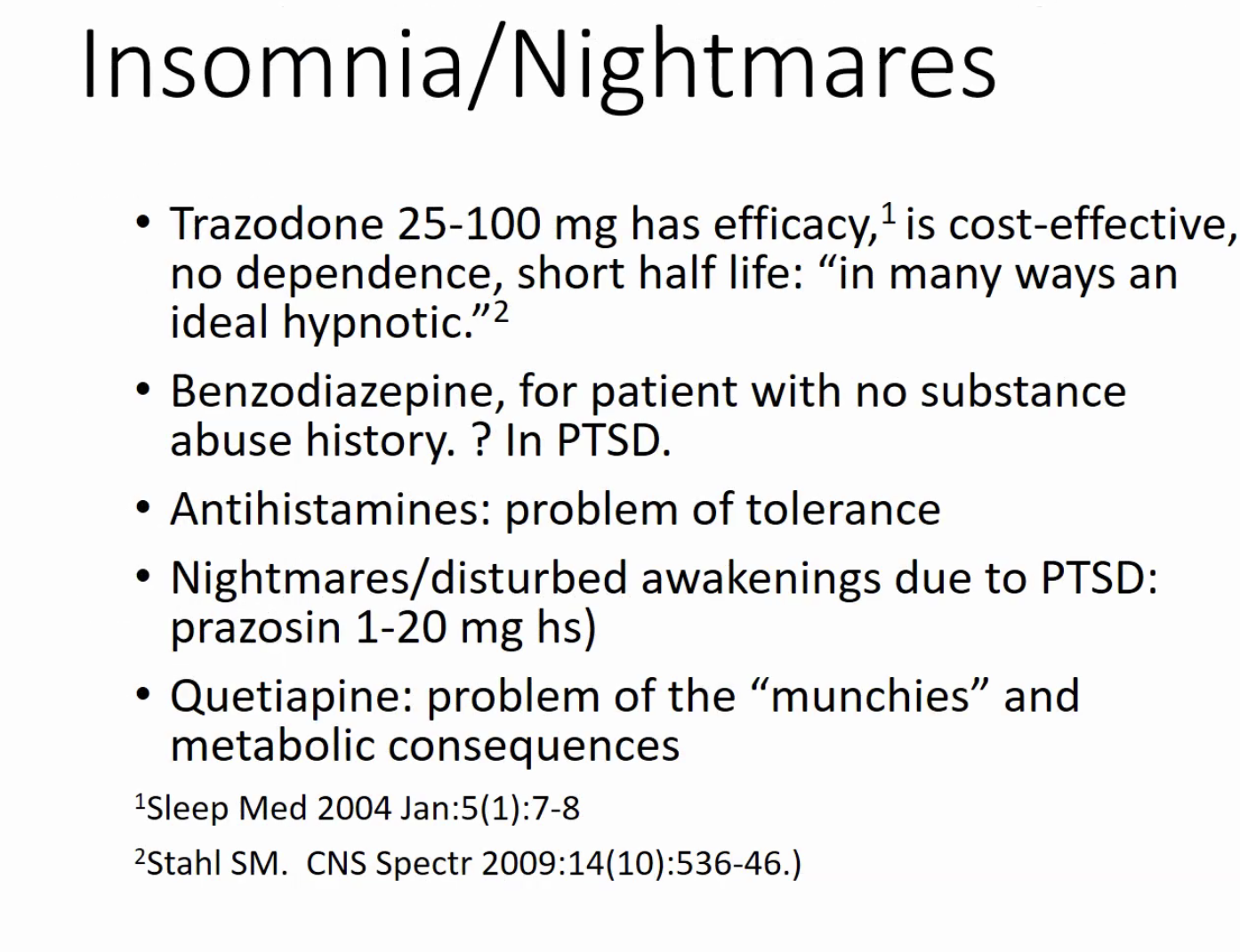
- doxepin low dose can also help
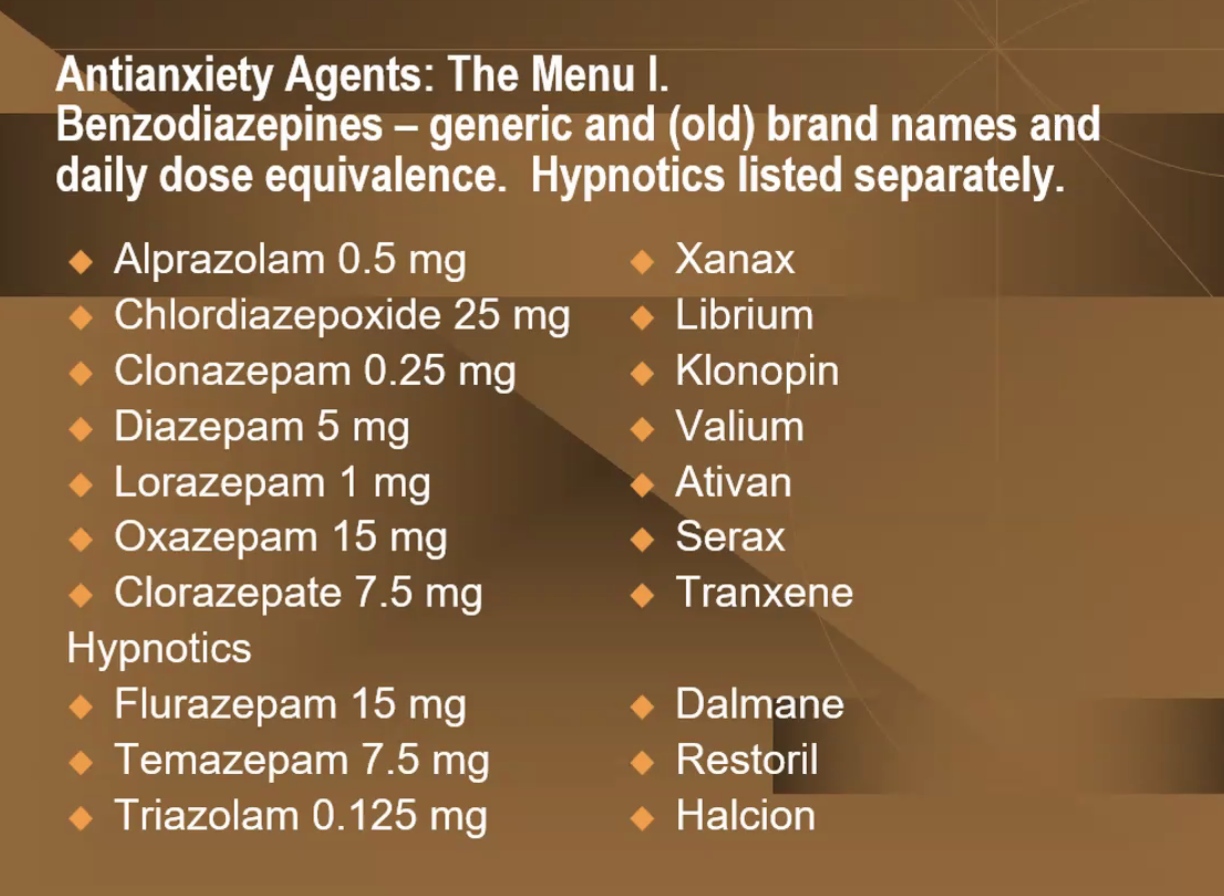
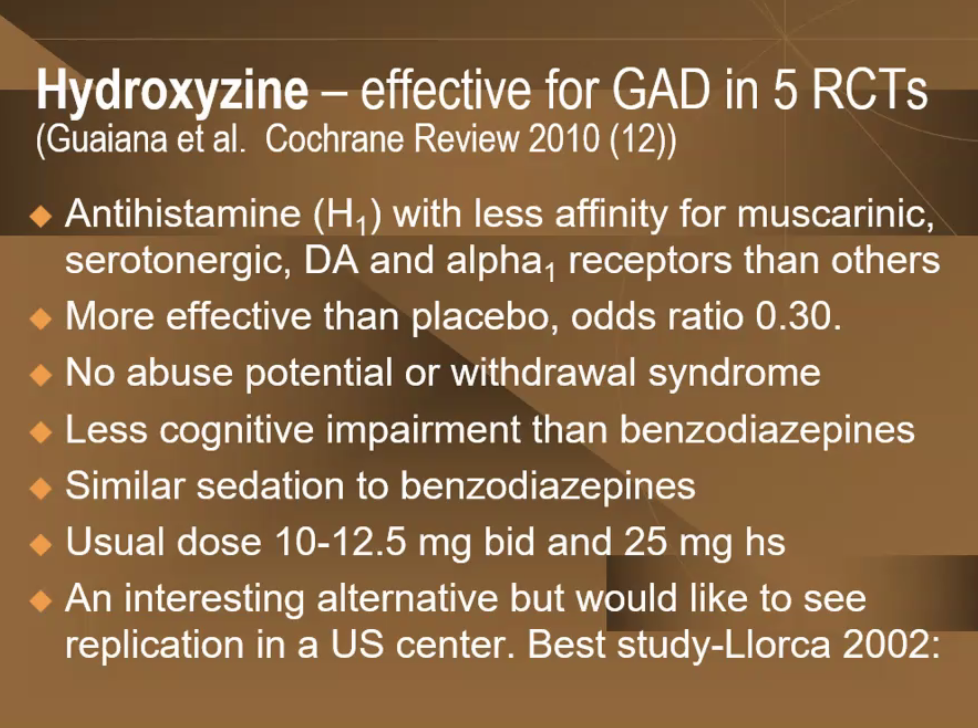
Anxiety
- SSRI/SNRI: first line
- second line: benzos
- useful for quick relief while waiting for SSRI to work