culture negative endocarditis
- related: ID
- tags: #id
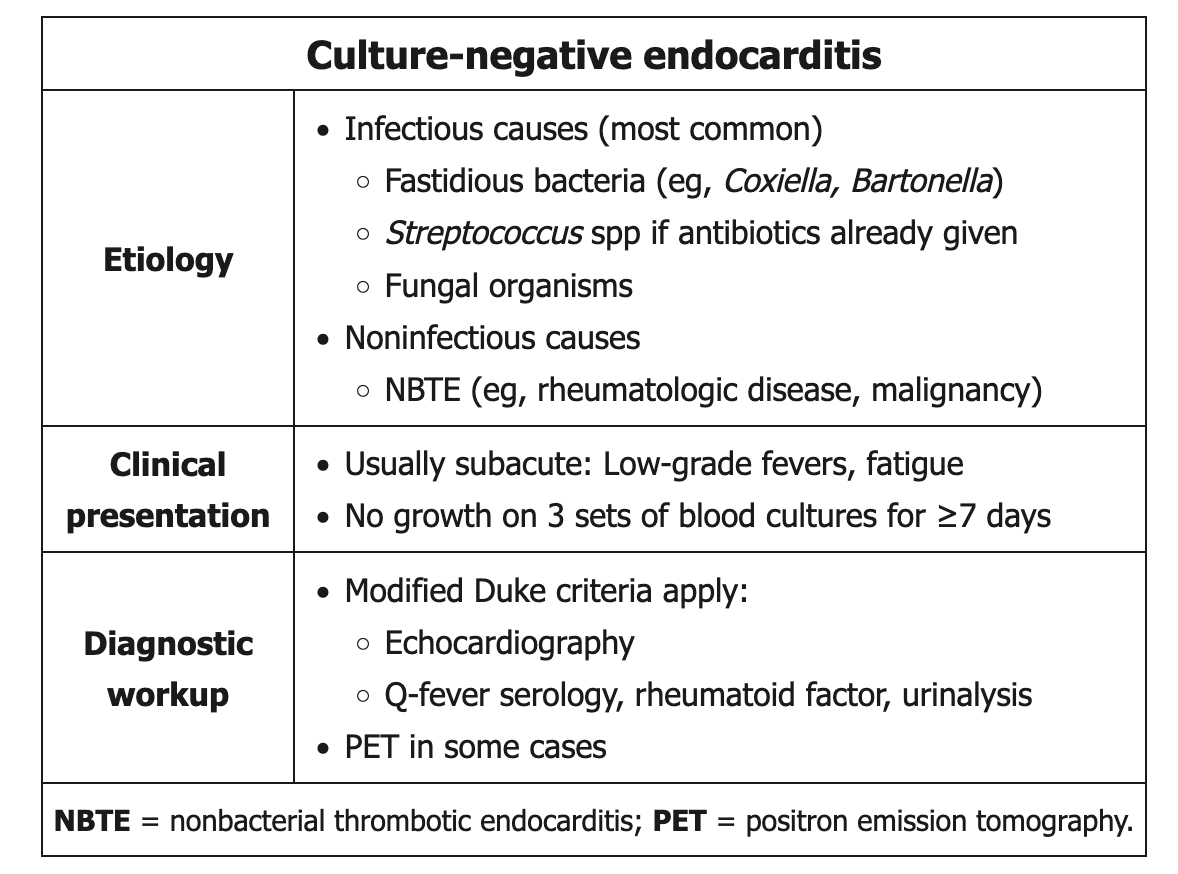
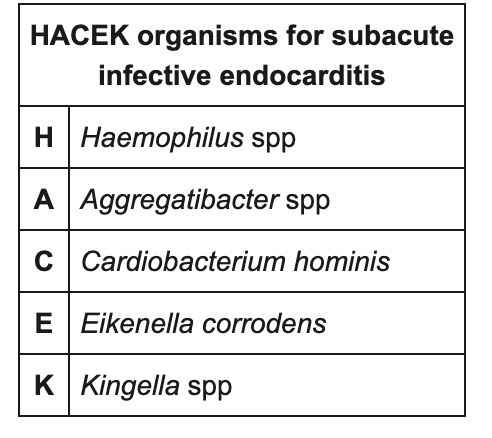
 This patient has multiple findings to suggest subacute infective endocarditis (ie, fatigue, low-grade fevers, splenic infarcts, murmur of aortic regurgitation). No growth on 3 sets of blood cultures after ≥7 days is consistent with culture-negative endocarditis (CNE), which suggests fungi or fastidious bacteria (eg, Coxiella burnetii, Bartonella spp, Tropheryma whippelii) as the most likely organism. HACEK bacteria are relatively easily detected by modern culture methods and are no longer considered a common cause of CNE.
This patient has multiple findings to suggest subacute infective endocarditis (ie, fatigue, low-grade fevers, splenic infarcts, murmur of aortic regurgitation). No growth on 3 sets of blood cultures after ≥7 days is consistent with culture-negative endocarditis (CNE), which suggests fungi or fastidious bacteria (eg, Coxiella burnetii, Bartonella spp, Tropheryma whippelii) as the most likely organism. HACEK bacteria are relatively easily detected by modern culture methods and are no longer considered a common cause of CNE.
In a large epidemiologic study of CNE, C burnetii was the most common organism identified; it is typically contracted by droplet exposure from infected livestock. Acute infection manifests as Q fever, which typically consists of pneumonia with flu-like symptoms and hepatitis but can be asymptomatic. Infective endocarditis can occur several months following acute infection; it is seen primarily in men age >40, pregnant women, and patients with underlying valvular pathology.
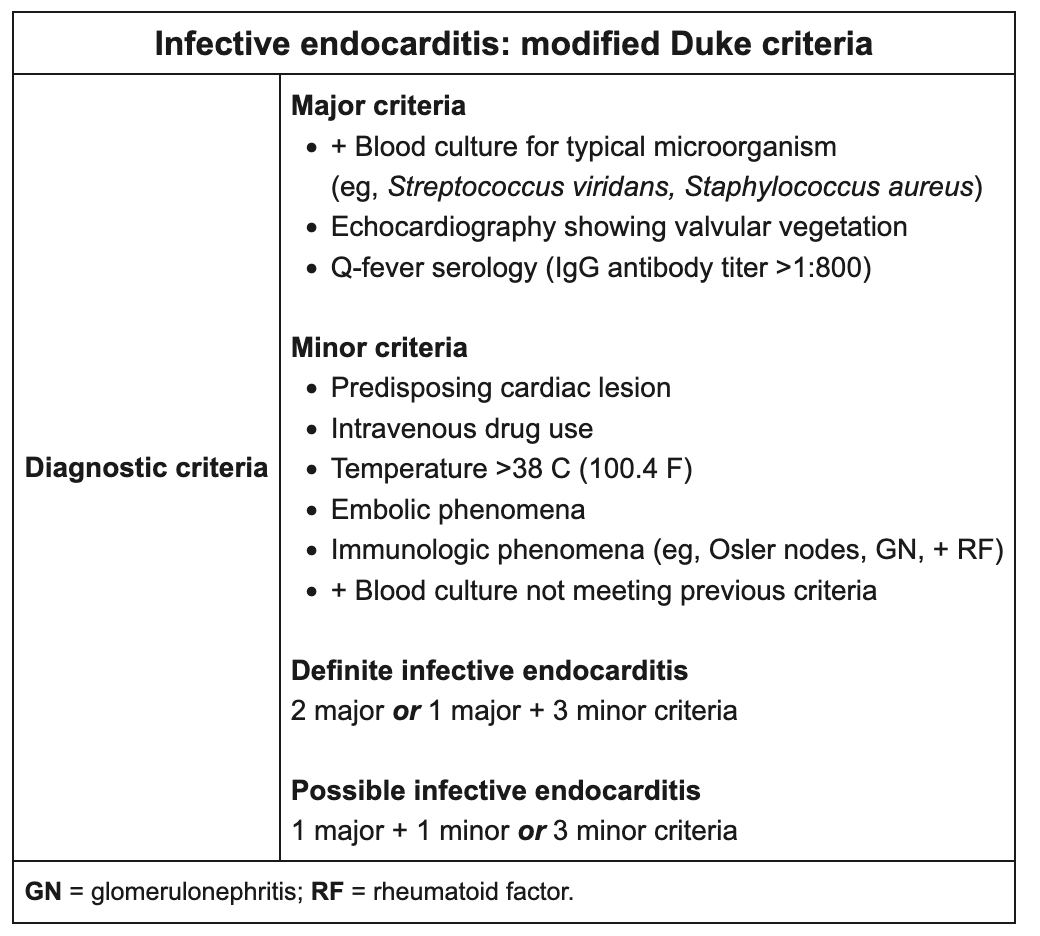
The modified Duke criteria are used for diagnosis; positive Q fever serology (IgG antibody titer >1:800) is considered a major clinical criterion. Initial diagnostic evaluation should include transthoracic or transesophageal **echocardiography** to identify valvular vegetations and perivalvular lesions. Positron emission tomography may also be helpful in suggesting infectious valvular pathology.