cryptococcus
- cryptococcus
- Starting HAART can cause IRIS
- Wait 5 weeks before starting HAART
Types:
- neoformans most common
- agathi: more tropical. Has decreased activity to fluconazole
- usually inhaled
Demographics
- BMT: less b/c ppx fluconazole
- alemduzumab: CD 52
- corticosteroids use
- calcineurin inhibitors have protected role against crypto
- Usually dormant for many years, reactivate with immunosuppression
Sx
- localized pneumonitis w or w/o sx
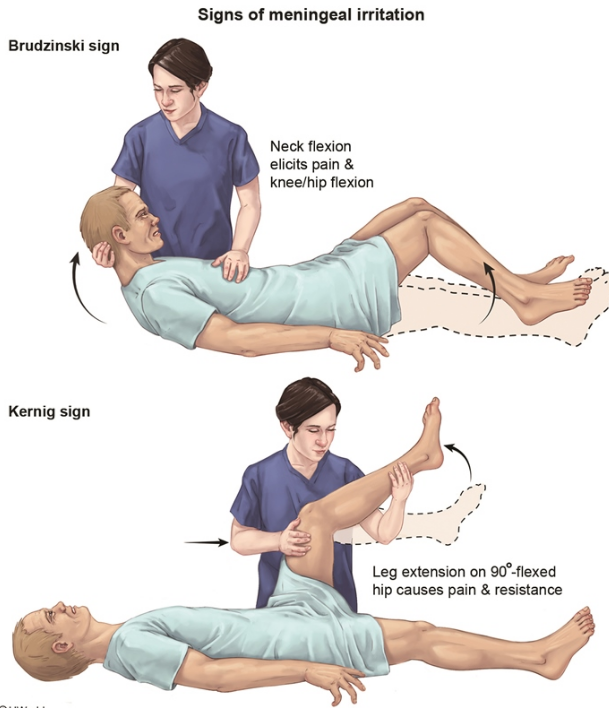
- dyspnea, cp, cough, fever, headache, meningitis sx, lethargy, confusion, photophobia
- subacute: 2-3 weeks
- brain: film around pia layer and prevents csf absorption: increased pressure. Sometimes traps around CN and can present with neurologic deficits
- assume dessimination on presentation, pulmonary and CNS involvement
- other organs: skin, soft tissue, bone, joints
Dx:
- cryptococcal antigen very good for dx
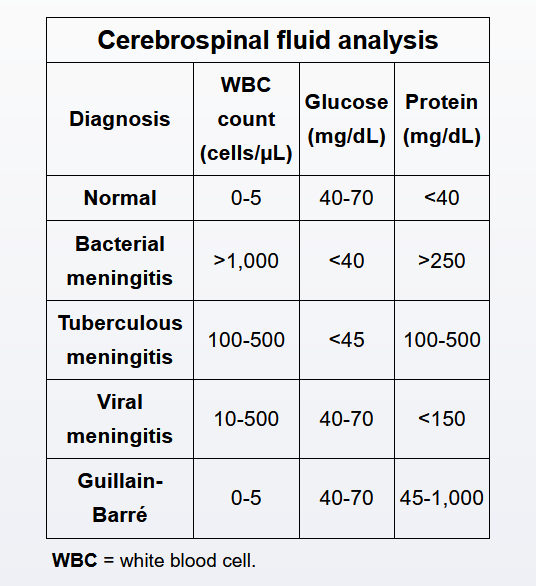
- LP: WBC not much changes, predominant monocytes, low/nl glucose, elevated protein
- no need to order fungal blood clx but send a fungal CSF culture b/c higher sensitivity
- titer and glucose in CNS has predicative value
- crypto antigen not good monitor tool (dead organism can cause positive antigen)
- negative culture and glucose better for monitoring
Mortality:
- CSF titer > 1000 or mental status changes = increased mortality
Treatment:
- induction with amphoteracin b liposomal form with flucytocin
- 2 week therapy with amphoteracin b then flucytosine for 8 weeks then suppressive therapy
- intracranial pressure: LP until CSF pressure <25. Improves survival
- reduce degree of immunosuppression: treat HIV, reduce immunosuppression in transplant. Don't change calcineurin inhibitors
- HIV: screen for crypto
- IRIS: improvement of immune function, reaction against organism = increased inflammatory process. Wait 8 weeks before HAART therapy
- severe sx: try prednisone
Cyrptococcus
Cryptococcus neoformans is a yeast that commonly causes opportunistic CNS infections in patients with AIDS (CD4 counts <100/mm3). Manifestations typically develop over 1-2 weeks and include fever, headache, and lethargy. Skin findings of papular lesions with central umbilication that resemble molluscum contagiosum are common. CSF studies usually reveal the following:
- Markedly elevated opening pressure, often >250-300 mm H2O
- Low leukocyte count (<50/mm3) (compared to other meningitides) with a lymphocytic predominance
- Elevated protein and low glucose
- Positive India ink preparation or cryptococcal antigen test
Patients with HIV who have cryptococcal meningitis require treatment in 3 stages as follows:
- Induction - amphotericin B and flucytosine for >2 weeks (until symptoms abate and CSF is sterilized)
- Consolidation - high-dose oral fluconazole for 8 weeks
- Maintenance - lower-dose oral fluconazole for >1 year to prevent recurrence
After 2 weeks of induction therapy, this patient has negative CSF cultures and no further symptoms; he can now be transitioned to oral fluconazole consolidation therapy.
Patients with AIDS who have cryptococcal meningoencephalitis often have dramatic cerebrospinal fluid fungal burdens (>1,000,000 yeast/mm3). The yeast and capsular polysaccharides can clog the arachnoid villi, which prevents cerebrospinal fluid outflow and increases intracranial pressure (ICP). Pressure elevations can often be dramatic (>250 mm H2O), resulting in headache, vomiting, visual changes, papilledema, and cranial nerve palsies. If untreated, brain herniation and death may occur. As such, patients with cryptococcal meningitis who develop recurrent symptoms of elevated ICP require serial lumbar punctures until symptoms abate. Occasionally, recalcitrant cases require more permanent treatment such as ventriculoperitoneal shunt.
Patients with AIDS who develop cryptococcal meningitis require the initiation of antiretroviral therapy (ART) to improve CD4 count and prevent recurrence. However, the early initiation of ART can be associated with life-threatening immune reconstitution inflammatory syndrome; ART initiation is typically delayed until there is sustained clinical improvement with treatment (generally after 2-10 weeks).
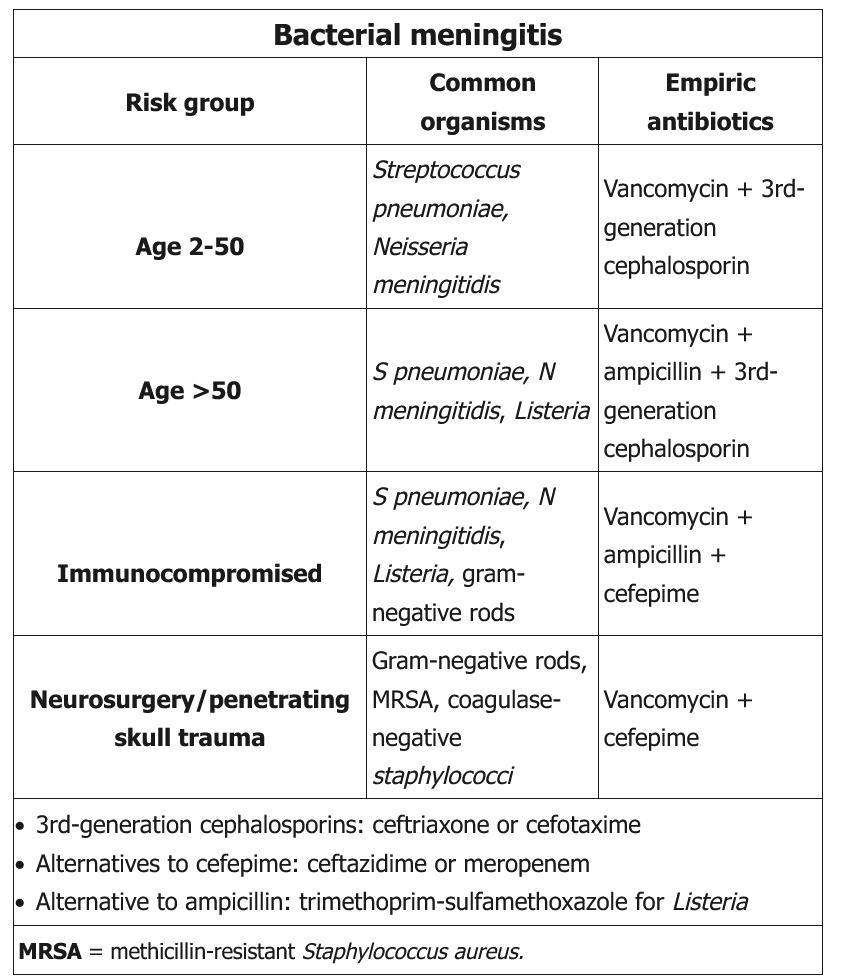
Dexamethasone is often added to the treatment of bacterial meningitis (eg, meningococcal meningitis) to reduce inflammation, morbidity, and risk of death. Dexamethasone is not recommended for the treatment of cryptococcal meningitis.