cocaine induced chest pain can be treated with benzodiazepines
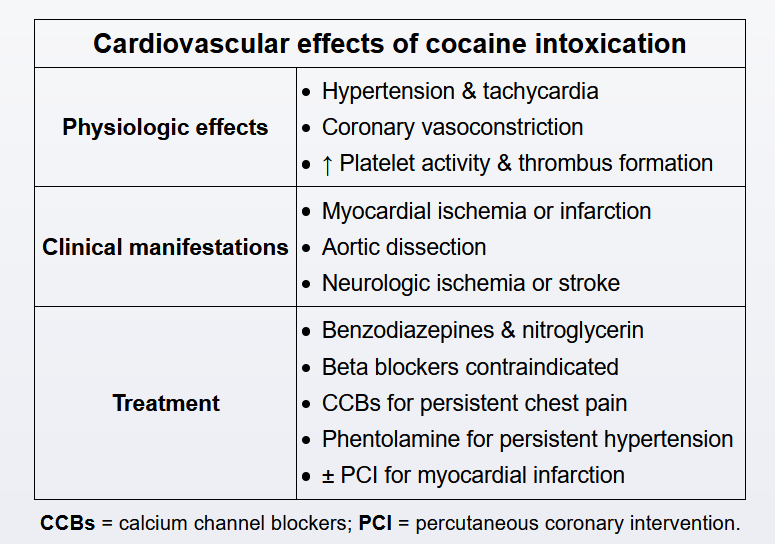
Although cocaine-related chest pain (CRCP) can occur due to noncardiac causes (eg, pneumothorax, hemorrhagic alveolitis or "crack lung"), clinicians should have a high index of suspicion for cardiovascular pathology. Most acute cardiovascular adverse effects of cocaine result from inhibition of the presynaptic reuptake of norepinephrine in the central nervous system, which leads to overstimulation of adrenergic receptors (eg, alpha-1, beta-1) and resulting tachycardia, increased myocardial contractility, arterial (including coronary) vasoconstriction, and hypertension. Because these effects lead to an increase in myocardial oxygen demand and a decrease in supply, myocardial ischemia and acute coronary syndrome (ACS) are common. Cocaine also activates platelets and supports thrombus formation, which further increases the risk of myocardial infarction and can lead to stroke. Cocaine-induced hypertension can also cause aortic dissection.
In patients with CRCP that is likely of cardiovascular etiology, benzodiazepines (eg, lorazepam, diazepam) are the preferred initial medication treatment. These drugs reduce sympathetic outflow to alleviate tachycardia and hypertension and improve myocardial ischemia. In addition, benzodiazepines calm cocaine-induced psychomotor agitation, which helps to decrease myocardial oxygen demand and provide further relief of myocardial ischemia. Nitroglycerin (sublingual or infusion) is also useful in alleviating hypertension (and myocardial ischemia) in these
Unless there is a contraindication (eg, high suspicion for aortic dissection), aspirin should be given early in the management of patients with CRCP. Clopidogrel should be given only when a diagnosis of ACS has been established (eg, ischemic ECG changes, elevated cardiac biomarkers).