clostridium difficile
- related: ID, fulminant clostridium difficile
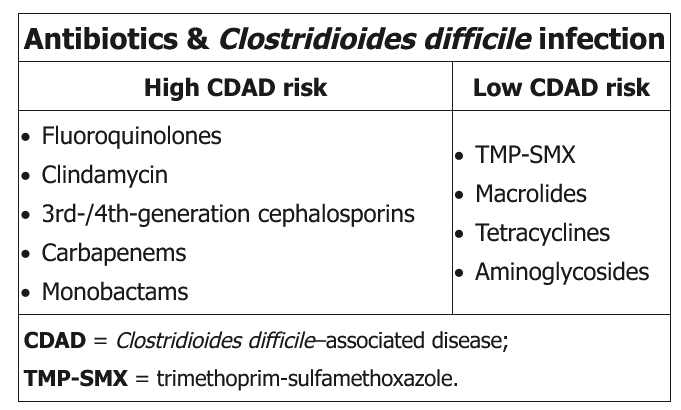
- Possibly restrict use of clindamycin, fluoroquinolones & cephalosporins
- Consider using aminoglycosides or trimethoprim-sulfamethoxazole instead of fluoroquinolones
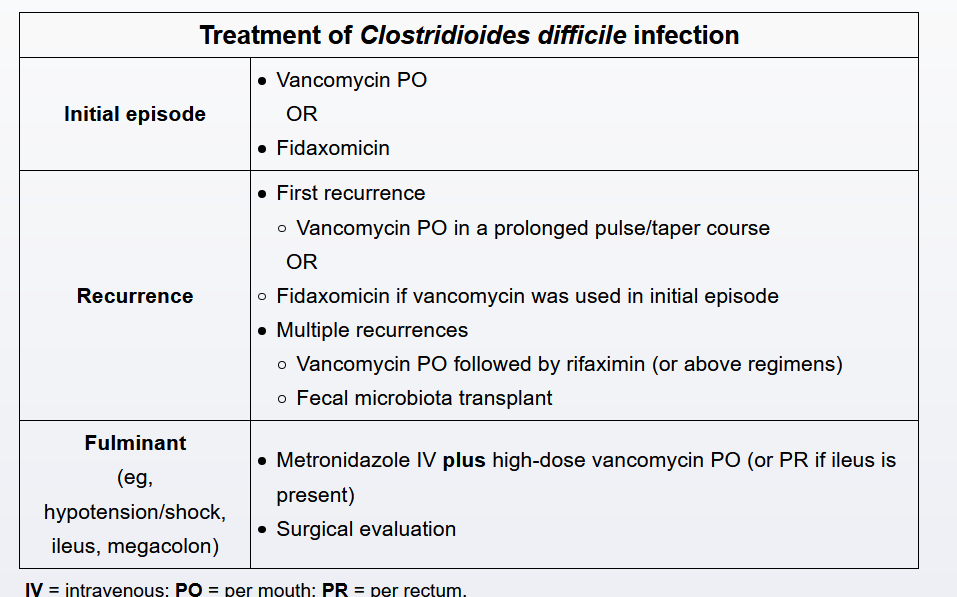
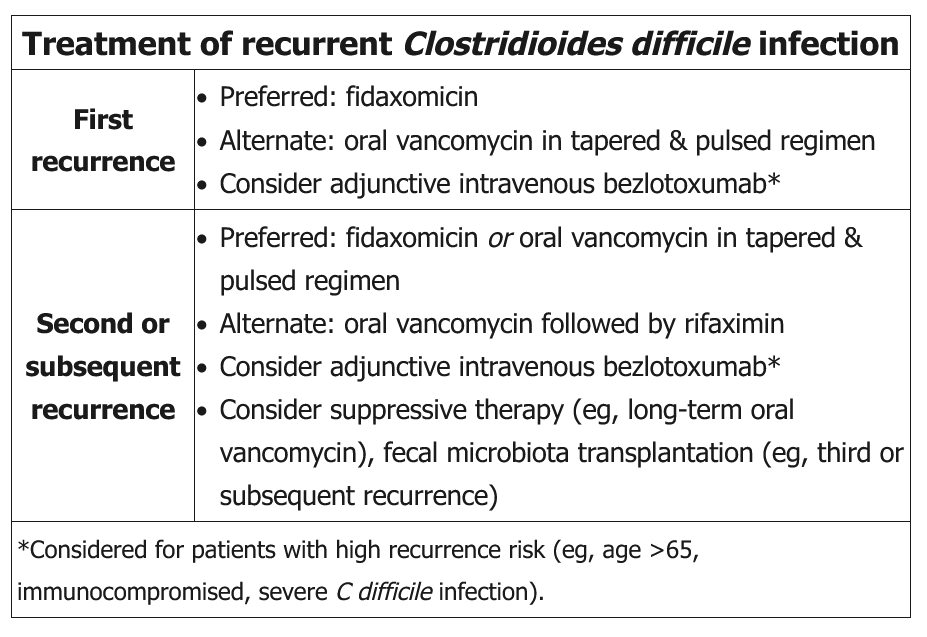
Recurrence of CDI is common, affecting approximately 15%-30% of patients whose condition initially responds to antimicrobial therapy, and is typically due to germination of persistent spores from the initial infection and not from drug resistance.
Fidaxomicin, in a standard (10-day) or an extended and pulsed regimen, is recommended for the management of an initial recurrence of CDI. A prolonged course of oral vancomycin given in a pulsed and tapered regimen (eg, 4 times daily for 10-14 days, twice daily for 7 days, daily for 7 days, every 2-3 days for 2-8 weeks) is an acceptable alternative. Adjunctive therapy with bezlotoxumab, a monoclonal antibody targeting C difficile toxin B, is considered for patients with an especially high recurrence risk (eg, age >65, immunocompromised status, severe CDI on presentation).
Oral vancomycin followed by rifaximin is an alternate treatment for further recurrences but is not recommended for the first CDI recurrence.