breast mass
- related: OBGYN, breast pain
- tags: #obgyn
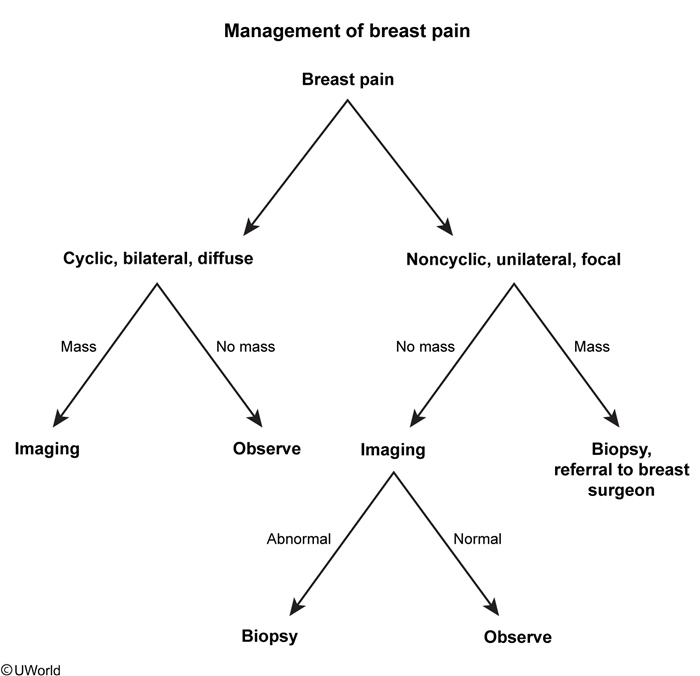
A firm, palpable breast mass with ill-defined borders is concerning for malignancy. Additional clinical features suggestive of malignancy include an immobile mass with associated lymphadenopathy, expressed nipple discharge, skin changes, or new-onset nipple inversion. However, history and physical examination are not sufficient for diagnosing or excluding malignancy in patients with breast masses, so diagnosis requires further evaluation with imaging.
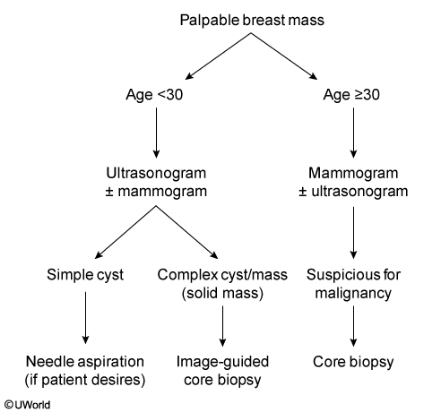
In patients age >30, first-line imaging is with mammography due to its ability to further characterize the mass and determine the need for biopsy. On mammography, cancer typically appears as a spiculated soft tissue mass with calcifications. Additional mammographic findings concerning for malignancy include architectural distortion and linear branching calcifications. If mammography shows the lesion but has no features suggestive of malignancy, an ultrasound can be performed (eg, targeted ultrasound) to further characterize the lesion (eg, solid, cystic). If imaging indicates possible malignancy, a core needle biopsy is performed to obtain tissue for histologic diagnosis, which will guide further management if malignancy is identified.