brainstem lesions
Careful assessment of a patient's signs and symptoms can help localize lesions within the central nervous system. Lesions of the thalamus or cortex are associated with sensory loss in the contralateral face and body. Cortical lesions are also associated with specific findings such as aphasia, neglect, or agraphesthesia. In contrast, brainstem lesions typically involve the cranial nerves and impair sensory perception over the ipsilateral face and contralateral body.
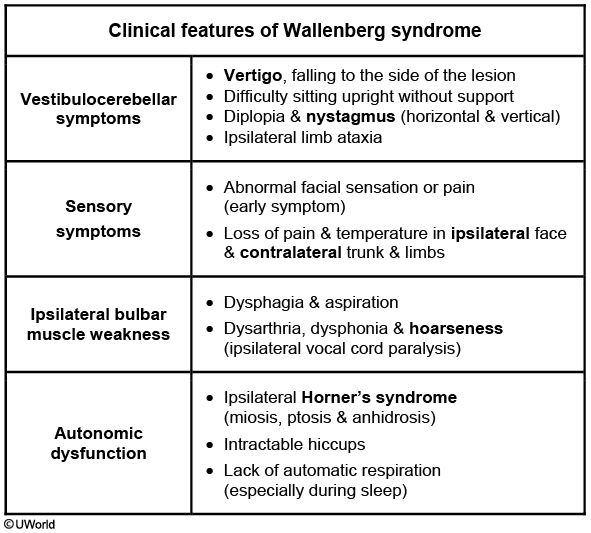
This patient's presentation suggests right-sided lateral medullary infarction (Wallenberg syndrome) most likely due to an occluded intracranial vertebral artery. Vestibulocerebellar findings are the most debilitating; patients may report difficulty feeding themselves and often overshoot targets due to ipsilateral limb ataxia. Sensory findings include loss of pain and temperature in the ipsilateral face and contralateral trunk/limbs. Patients typically have sparing of voluntary motor function in the face and body. Diagnosis is made via magnetic resonance imaging; acute treatment usually involves intravenous thrombolytics (eg, tissue plasminogen activator).
Gertsmann syndrome
Damage to the dominant parietal lobe, especially the inferior parietal lobe, presents as Gerstmann syndrome. The patients have difficulty in performing simple arithmetic tasks (acalculia), inability to name individual fingers (finger agnosia), impaired writing (agraphia) and right/left confusion (difficulty in identifying or distinguishing the right or left side of the body).
Almost 90% of right-handed patients and 60% of left-handed patients have a left hemispheric dominance for speech and language functions. The patient in the above scenario appears to be suffering from construction apraxia. This is seen with the involvement of parietal lobes, and is much more pronounced with lesions of the right parietal hemisphere (nondominant parietal lobe). Patients have marked difficulty in copying simple line drawings. They may also experience difficulty in wearing clothes, and appear to struggle while attempting to get into a coat or pants. This is known as dressing apraxia, which is seen with bilateral or right-sided (nondominant) parietal lobe lesions. Confusion is also seen in patients with lesions of the nondominant parietal lobe.
Temporal lobe
Lesions of the nondominant temporal lobe can cause visual disorders (homonymous upper quadrantanopia) and impaired perception of complex sounds (auditory agnosia).
Dominant temporal lobe lesions, in addition to having homonymous upper quadrantanopia, almost always involve the language functions, and lead to aphasia. Wernicke's aphasia is usually seen in patients with dominant temporal lobe lesions. It is characterized by the impairment in comprehension of spoken or written language. Patients have difficulty in expressing their thoughts in a meaningful manner. Apraxia is not seen in temporal lobe lesions.
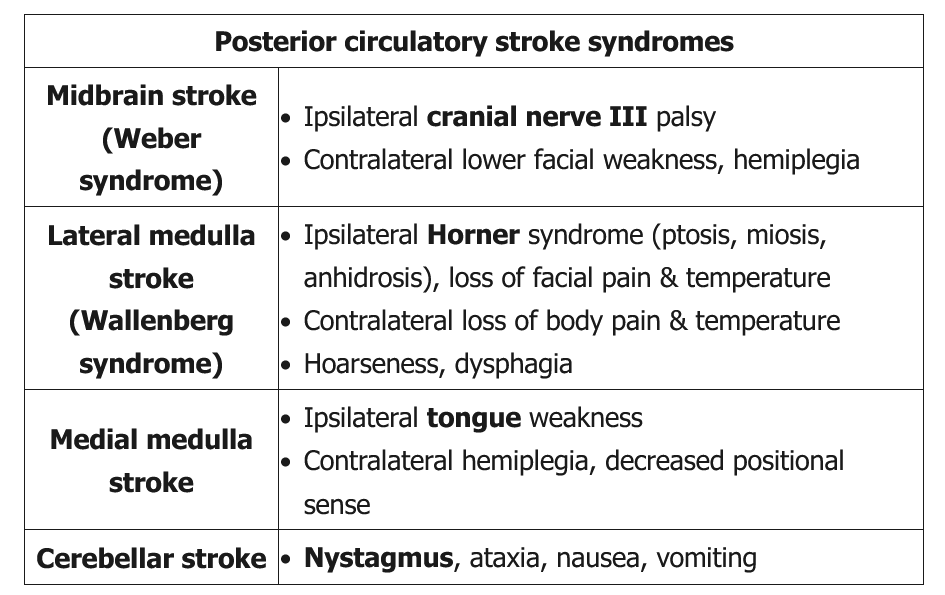
CN involvement can help with localization based on the origin within the brainstem:
- Midbrain (CNs III-IV): oculomotor (III), trochlear (IV)
- Pons (CNs V-VIII): trigeminal (V), abducens (VI), facial (VII), vestibulocochlear (VIII)
- Medulla oblongata (CNs IX-XII): glossopharyngeal (IX), vagus (X), spinal accessory (XI), hypoglossal (XII)
The olfactory (CN I) and optic (CN II) nerves originate in the cerebrum and are not affected in brainstem stroke.