brachial plexopathy
- related: Neurology
- tags: #neurology
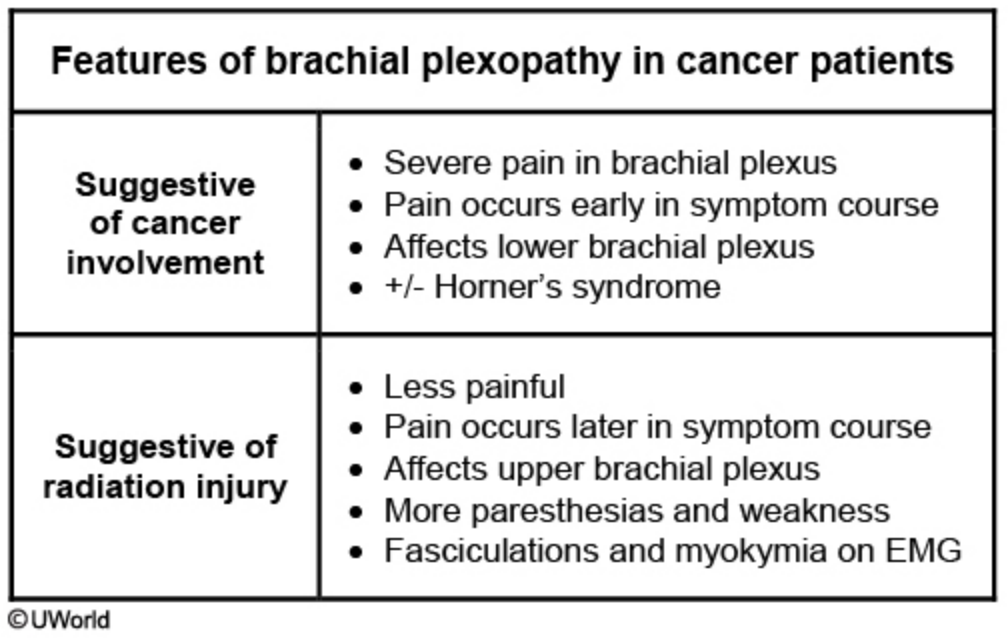
This patient’s presentation is consistent with brachial plexopathy, which is most commonly associated with breast and apical lung cancer. Brachial plexopathy can occur from direct cancer invasion or from radiation injury. Patients typically develop gradual weakness in the brachial plexus distribution; the above table summarizes the differences between cancer-induced and radiation-induced brachial plexopathy.
- Direct cancer invasion of the plexus nerves usually presents with more severe pain at symptom onset, involves the lower plexus, and is associated with Horner syndrome.
- Radiation injury presents with pain later in the symptom course, affects the upper plexus, and has more paresthesias and weakness.
Electromyography can also help distinguish between the 2 conditions (i.e., fasciculations and myokymia are more likely to be seen in radiation plexitis). This patient’s lower plexus pain and Horner syndrome suggests cancer-induced rather than radiation-induced plexopathy.