bacterial vaginosis
- related: STDs
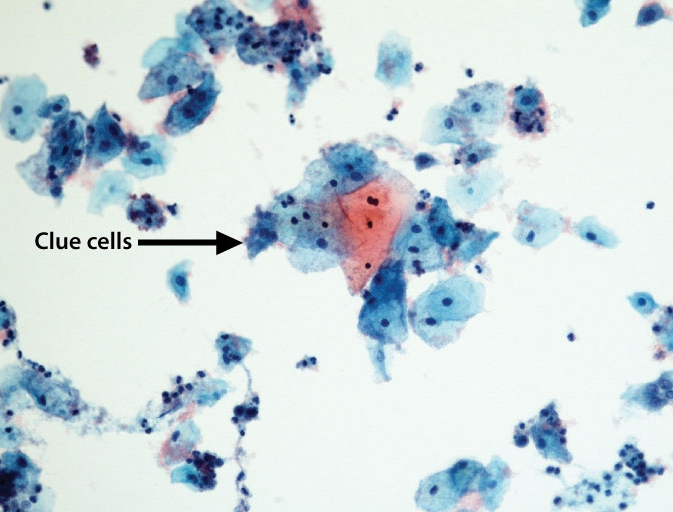
This patient has bacterial vaginosis (BV) based on a thin, malodorous vaginal discharge and clue cells (eg, stippled epithelial cells) on wet mount microscopy. BV occurs when the concentration of hydrogen peroxide-producing lactobacilli in the vagina decreases and the vaginal pH increases, resulting in an overgrowth of anaerobic vaginal flora (eg, Gardnerella vaginalis, Mycoplasma hominis). The decreased lactobacilli concentration that leads to BV can be due to hormonal fluctuation (eg, pregnancy), menses, sexual activity, antibiotic use, or douching.
BV is diagnosed when 3 of the following criteria are present:
- Homogeneous vaginal discharge
- Vaginal pH >4.5
- Amine odor after application of potassium hydroxide
- Clue cells (epithelial cells covered in bacteria) on wet mount microscopic examination
Patients with symptomatic BV are treated with oral or vaginal metronidazole or clindamycin as these antibiotics provide anaerobic coverage and improve the vaginal microflora balance; however, recurrence is common.
Bacterial vaginosis (BV) in pregnancy is associated with complications including spontaneous abortion, preterm premature rupture of membranes, preterm labor, chorioamnionitis, and postpartum endometritis (Choice E). However, screening and treating patients (symptomatic or asymptomatic) for BV does not decrease the incidence of these complications (Choice A). During pregnancy, only patients who have symptomatic BV are treated with metronidazole or clindamycin; the treatment goal is symptom relief rather than prevention of adverse obstetric outcomes.