autoimmune hemolytic anemia
- related: Hemeonc
- tags: #hemeonc
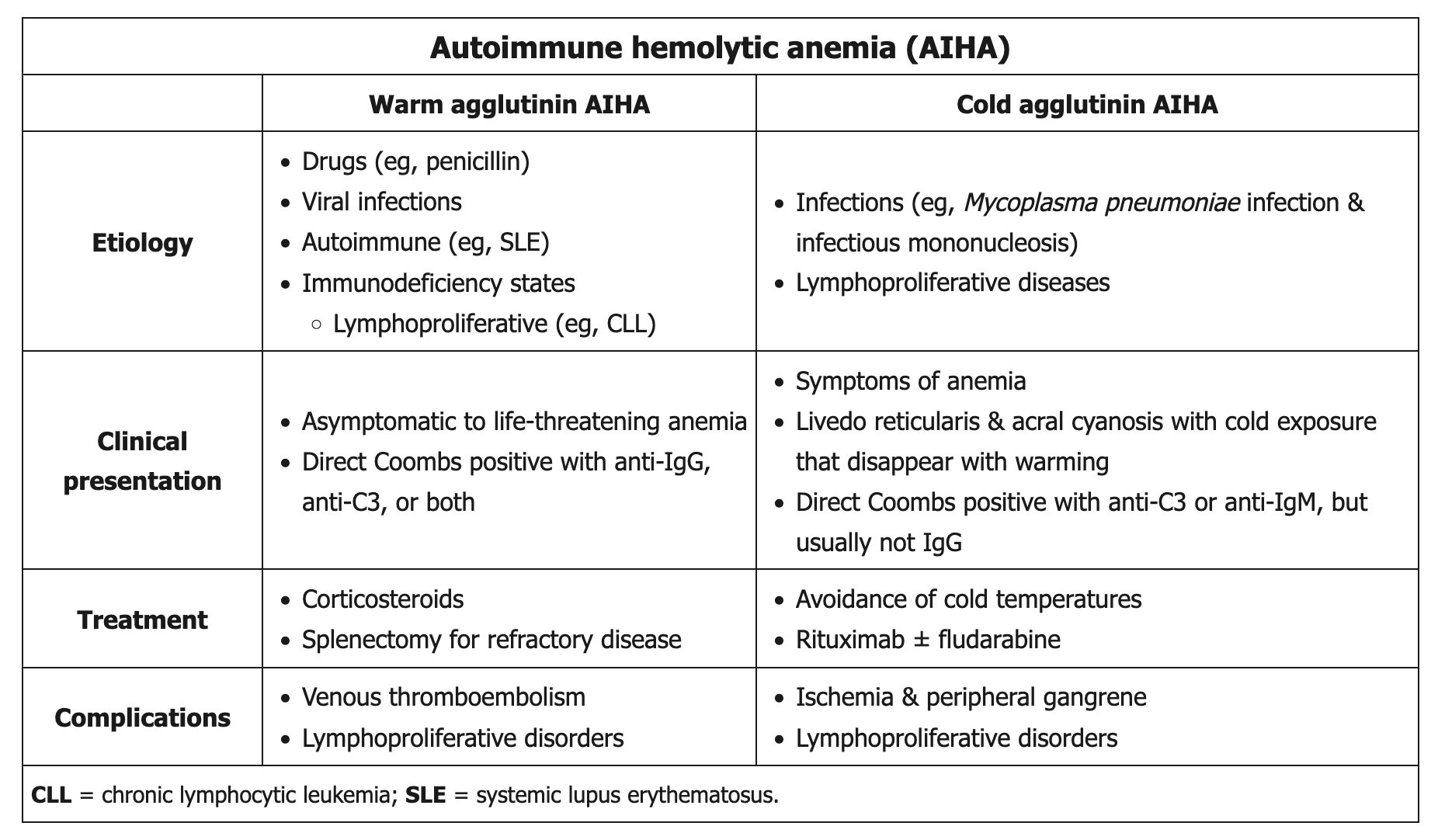 This patient's presentation suggests autoimmune hemolytic anemia (AIHA), a complication in about 10% of patients with systemic lupus erythematosus (SLE). AIHA is due to autoantibodies (warm agglutinins or IgG antibodies and cold agglutinins or IgM antibodies) destroying red blood cells. Nearly 80% of cases of AIHA are due to warm agglutinin disease. Patients typically present with signs and symptoms of anemia.
This patient's presentation suggests autoimmune hemolytic anemia (AIHA), a complication in about 10% of patients with systemic lupus erythematosus (SLE). AIHA is due to autoantibodies (warm agglutinins or IgG antibodies and cold agglutinins or IgM antibodies) destroying red blood cells. Nearly 80% of cases of AIHA are due to warm agglutinin disease. Patients typically present with signs and symptoms of anemia.
Laboratory findings include decreased hemoglobin and serum haptoglobin, increased indirect bilirubin and lactate dehydrogenase, reticulocytosis, and spherocytosis on peripheral smear due to partial phagocytosis of IgG-coated red blood cells. Spherocytosis results in increased mean corpuscular hemoglobin concentration. Elevated mean corpuscular volume (MCV) is due to the reticulocytosis. Diagnosis is established by a positive direct antiglobulin (Coombs') test.
Steroids are first-line treatment for SLE-associated AIHA, with rapid tapering after the hematocrit increases and reticulocytosis decreases. Splenectomy is indicated if there is no response to steroids or in patients who require high-dose steroids to maintain response.