antibiotic prophylaxis for secondary prevention of rheumatic fever
- related: ID
- tags: #id
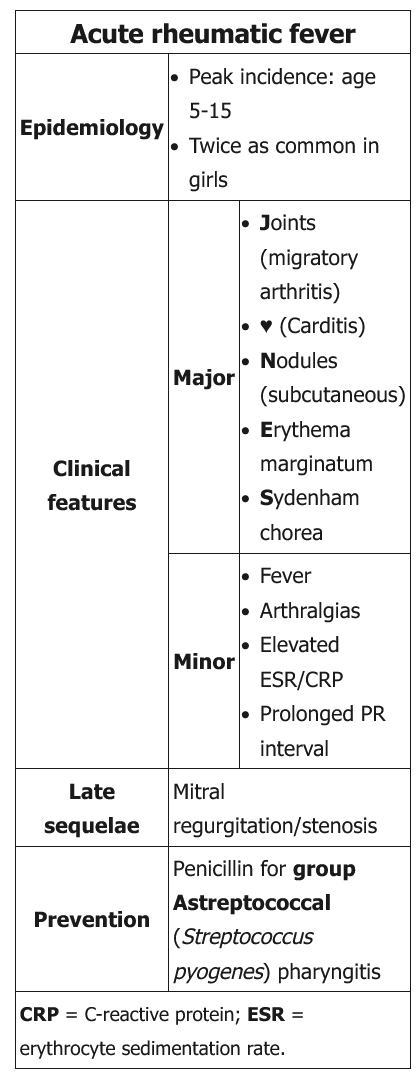
This patient's childhood history of a febrile illness with movement disorder (chorea) is consistent with previous rheumatic fever complicated by persistent valvular disease (mitral stenosis). Rheumatic fever occurs as a complication of group A beta-hemolytic Streptococcus (GAS) pharyngitis; the initial acute disease and recurrences can be characterized by fever, arthritis, chorea, and heart failure. This patient's current presentation is not consistent with rheumatic fever recurrence; however, the sore throat raises suspicion for GAS pharyngitis.
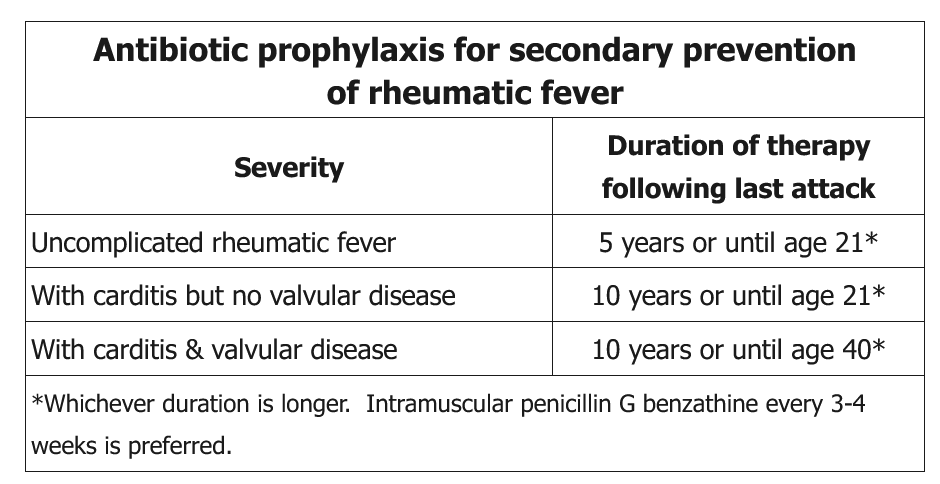
With repeated exposure to GAS, patients with prior rheumatic fever are at high risk for recurrent rheumatic fever and consequent progression of rheumatic heart disease. Therefore, they should receive continuous antibiotic prophylaxis to prevent GAS pharyngitis. Long-acting penicillin G benzathine given intramuscularly every 3-4 weeks is the preferred approach for secondary prevention of rheumatic fever recurrence, and the duration of antibiotic prophylaxis depends on the severity of underlying rheumatic heart disease (presence or absence of carditis and valvular disease). The first dose of intramuscular penicillin would also treat any current GAS colonization/infection.
Oral penicillin V potassium is an acceptable treatment option for acute GAS pharyngitis (primary prevention of rheumatic fever). It is also an alternate treatment for secondary prevention of rheumatic fever recurrence; however, due to increased failure rates with orally administered antibiotics, intramuscular penicillin G is preferred.
Regardless of whether this patient was previously on antibiotics for rheumatic fever, she should receive an intramuscular dose of penicillin now and should be on continuous antibiotic prophylaxis until age 40 (given her valvular disease).