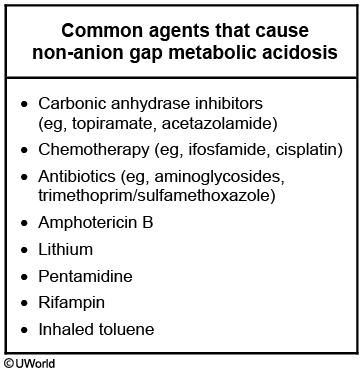
anion gap metabolic acidosis
- related: Nephrology, nonanion gap metabolic acidosis NAGMA
- tags: #nephrology
Etiologies

CAT MUDPILES
- CO/cyanide/congenital heart failure
- aminoglycosides
- toluene (glue sniffing)/teophylline
- Methanol
- Uremia: BUN elevation
- DKA, alcoholic ketoacidosis, starvation ketoacidosis
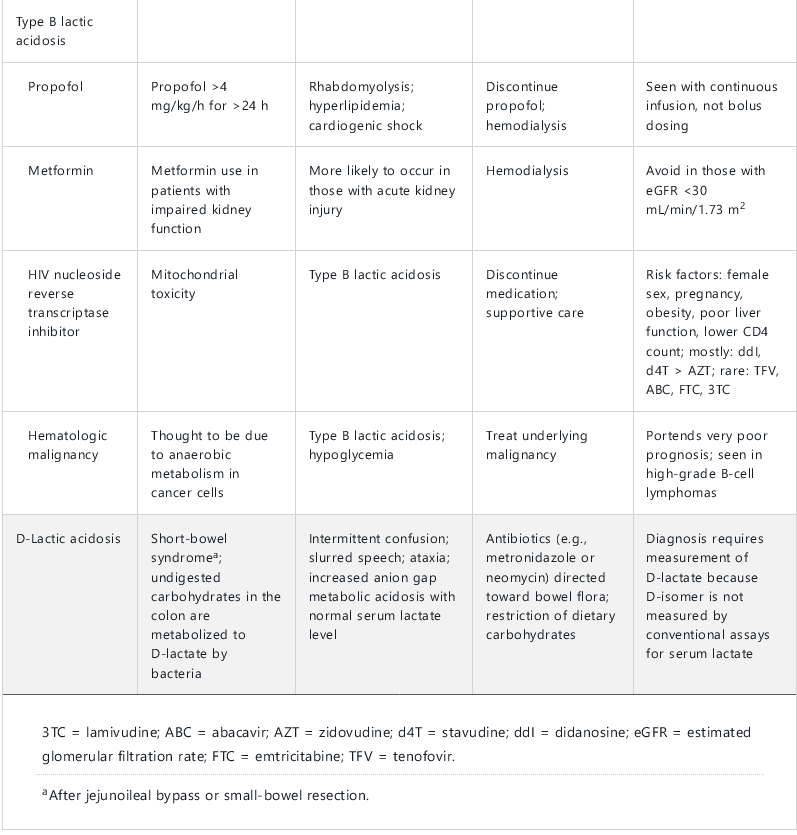
- Paracetamol/acetaminophen, paraldehyde, pyroglutamic acidosis, polyethylene glycol (miralax, metabolizes to lactic acid; versed, in the preparation, in neuro icu), propofol related infusion syndrome from high TG (Brugada syndrome)
- iron, isoniaziad, inborn errors of metabolism
- lactic acidosis
- ethanol/ethylene glycol toxicity (use wood's lamp)
- salicylates
Alternative: GOLD MARK
- G: glycol
- O: oxoproline: metabolite of acetamiophen
- L: lactate
- D: D lactate
- M: methanol
- A: ASA
- R: renal failure, correponds to uremia. Bicarb loss usually before stage 5 and regresses after stage 5. AG happens more in stage 5 when kidney is unable to excrete ammonia and other titratable acids. Uremia could also be related to steroids and GI bleed.
- K: ketoacidosis
Diagnosis
- plasma osmolar gap may be helpful to determine etiology
Diabetic ketoacidosis
Diabetic ketoacidosis usually presents with an increased anion gap metabolic acidosis due to accumulation of β-hydroxybutyrate and acetoacetate, although it may present with a normal anion gap due to excretion of ketoacids. Compensatory hyperventilation is characterized by increased tidal volume rather than increase in respiratory rate. Urine dipstick assays for ketones detect acetoacetate using the nitroprusside assay; however, β-hydroxybutyrate is the dominant ketoacid in diabetic ketoacidosis, so urine dipstick results can be falsely negative or underestimate the total ketone load.
Alcoholic ketoacidosis
Alcoholic ketoacidosis occurs in patients with chronic ethanol abuse who typically have a history of recent binge drinking, little food intake, and persistent vomiting. Liver chemistry test abnormalities may be present due to concomitant alcoholic hepatitis. Treatment with intravenous saline and intravenous glucose typically results in rapid resolution of ketones due to induction of insulin secretion and suppression of glucagon release. For patients with chronic malnutrition related to alcohol use, thiamine should be administered before glucose to decrease the risk of precipitating Wernicke encephalopathy.
Starvation
Starvation ketoacidosis (due to lipolysis with formation of free fatty acids and conversion into ketones) also causes ketonuria and an osmolar gap. However, these patients typically have a high AGMA.
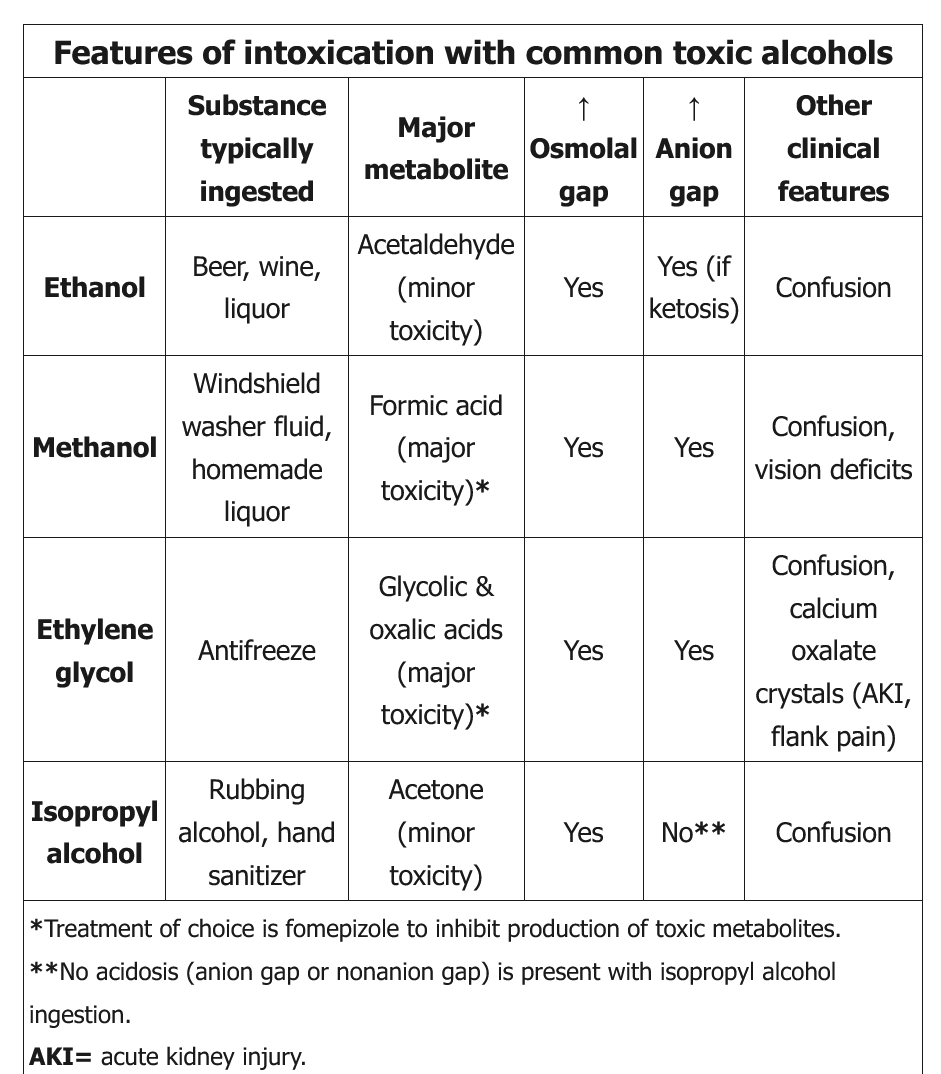
Ethanol
Ethanol is the most common cause of an elevated osmolar gap; the contribution of ethanol to serum osmolality can be calculated by dividing the serum ethanol level by 4. Isolated ethanol ingestion causes only an elevated osmolar gap (without AGMA). By contrast, alcoholic ketoacidosis occurs when patients with long-standing alcohol abuse and poor nutritional status have an episode of binge drinking, leading to ketosis (with AGMA). This patient's normal blood alcohol level and anion gap rule out alcoholic ketoacidosis.
Ethylene glycol
This patient has typical findings of ethylene glycol toxicity, including central nervous system depression, an increased anion gap metabolic acidosis, and an increased plasma osmolar gap.
Because laboratory confirmation of ethylene glycol intoxication may take days, empiric therapy with fomepizole and aggressive fluid resuscitation with crystalloids (250-500 mL/h intravenous initially) should be instituted in all cases to increase kidney clearance of the toxin and to limit deposition of oxalate in the renal cortex. Hemodialysis to clear the alcohol and toxic metabolites should be instituted in the context of any organ-specific toxicity (central nervous system depression, acute kidney injury, systemic collapse), severe acidemia, or very large ingestions.
Isopropyl alcohol
Isopropyl alcohol, like ethanol, is a central nervous system depressant. It is rapidly metabolized by alcohol dehydrogenase to the ketone acetone, leading to elevated serum and urine ketone measurements. Some laboratories measure beta-hydroxybutyrate concentrations as a substitute for serum ketones, leading to a falsely low measurement in patients with isopropyl alcohol ingestion. Unlike methanol and ethylene glycol, isopropyl alcohol does not cause high AGMA and does not have toxic metabolites causing further damage (eg, blindness, renal failure). It does cause increased osmolar gap.
Massive ingestions can cause respiratory depression and hypotension. Treatment is mainly supportive with intravenous fluids, pressors, and mechanical ventilation; hemodialysis can be initiated in severe cases. Fomepizole and gastrointestinal decontamination are usually not helpful.
Propylene glycol
Propylene glycol, a solvent used to enhance the solubility of various intravenously administered medications, causes an increased anion gap metabolic acidosis through its acid metabolites, L-lactate and D-lactate. An increased osmolal gap accompanies the increased anion gap metabolic acidosis seen with propylene glycol. This patient's clinical history and lack of lactic acidosis are not consistent with propylene glycol toxicity.
Salicylate
Salicylate toxicity most commonly presents in adults as respiratory alkalosis or with features of both respiratory alkalosis and increased anion gap metabolic acidosis. This patient has appropriate respiratory compensation for the metabolic acidosis, not respiratory alkalosis, making salicylate toxicity unlikely.
- sx: tinnitus, nausea, abd pain
- treat with bicarb, alkalinize the blood as much as possible, the rest with rest in to urine and bind salicylates, and pee out
- do not use acetazolamide: this doens't have increased serum bicarb
- do dialysis if salicylate > 100 or having sx + 80
- low pH < 7.2
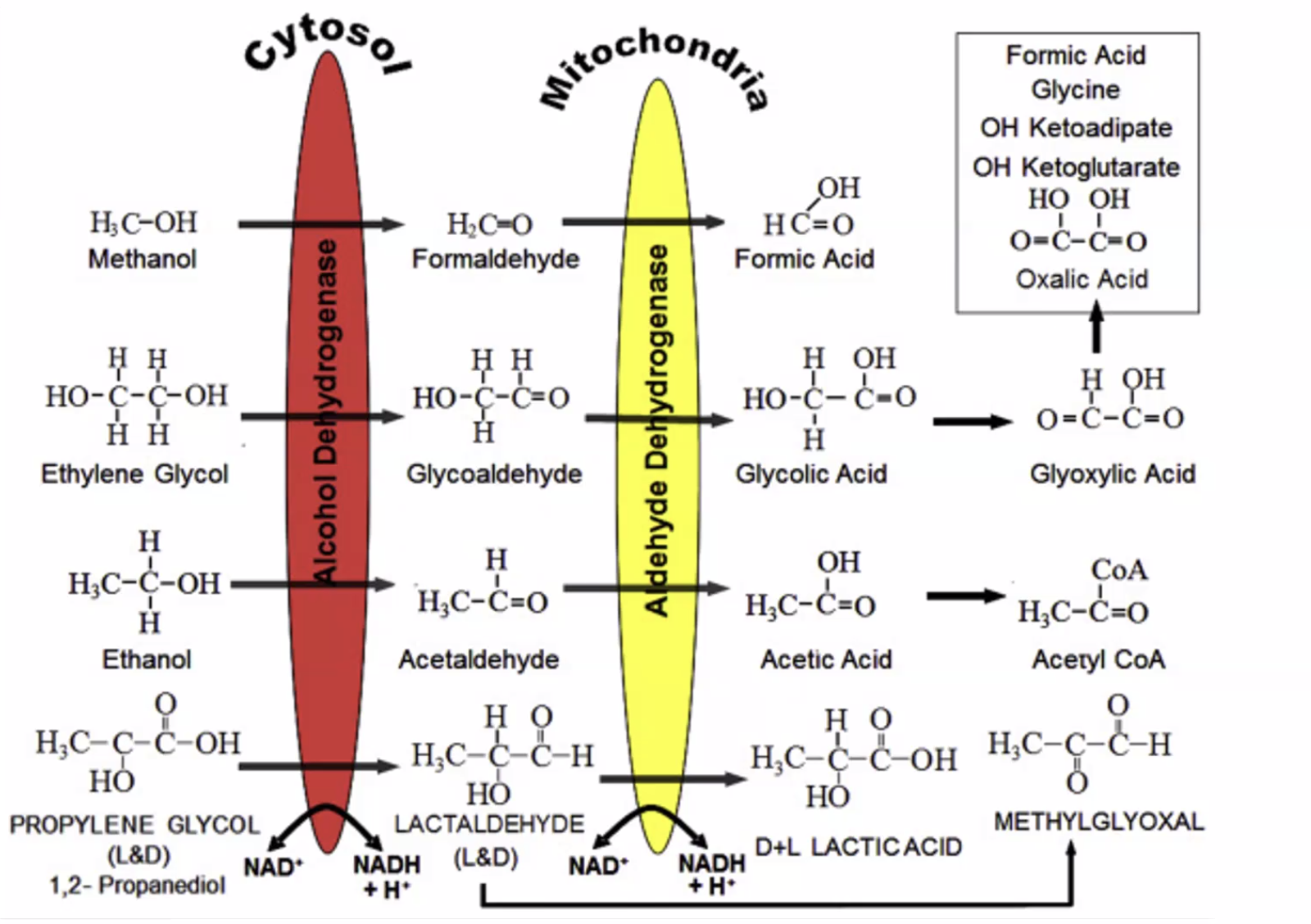
- ethanol does not have high AG because acetic acid is rapidly converted to acetyl coa
- isopropyl alcohol: osmolar gap but no AG acidosis. Rapidly changed to acetone
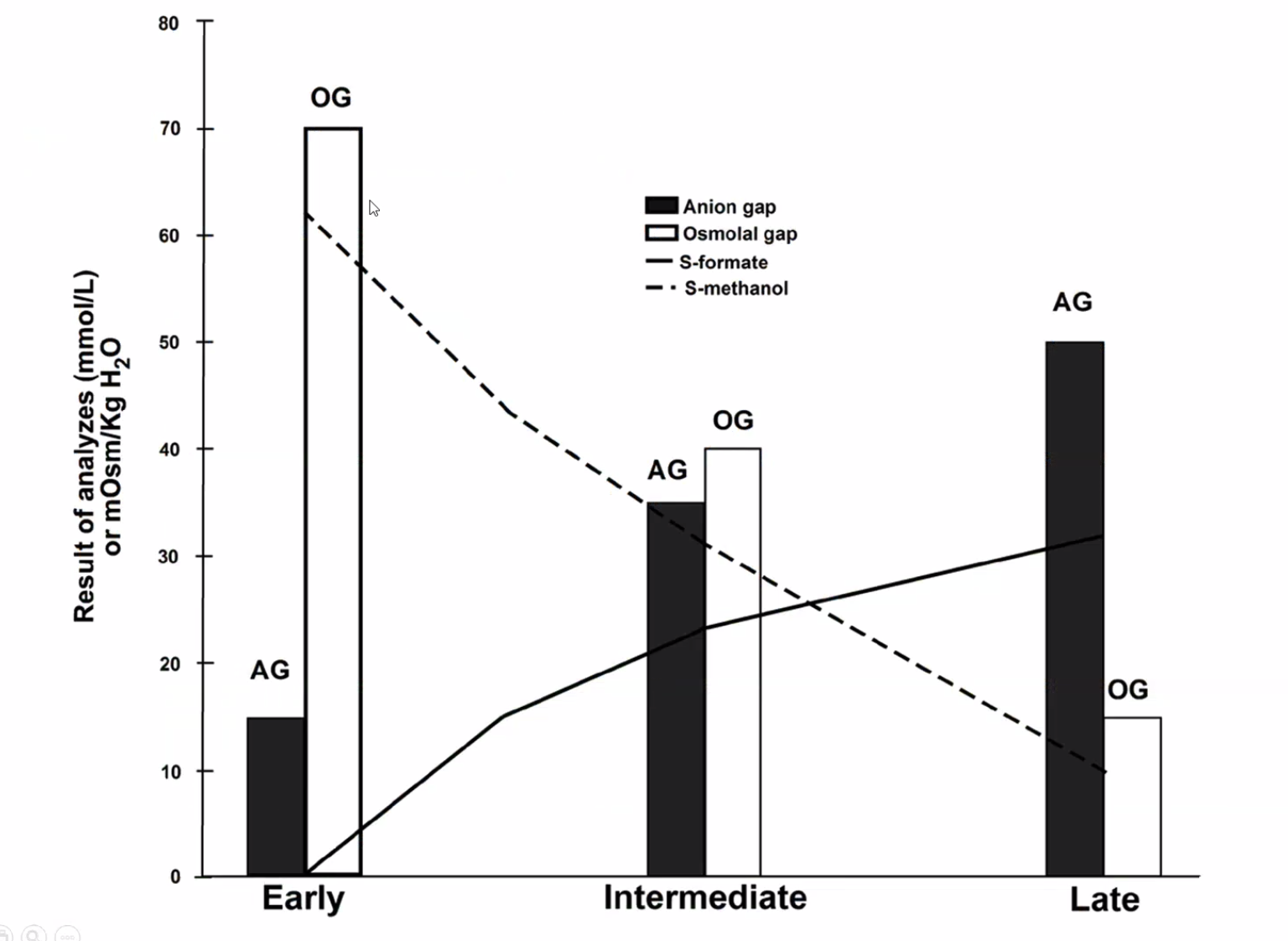
- pt can have normal AG but high osmolar gap in the beginning as things are metabolized over time.