Uterine bleed
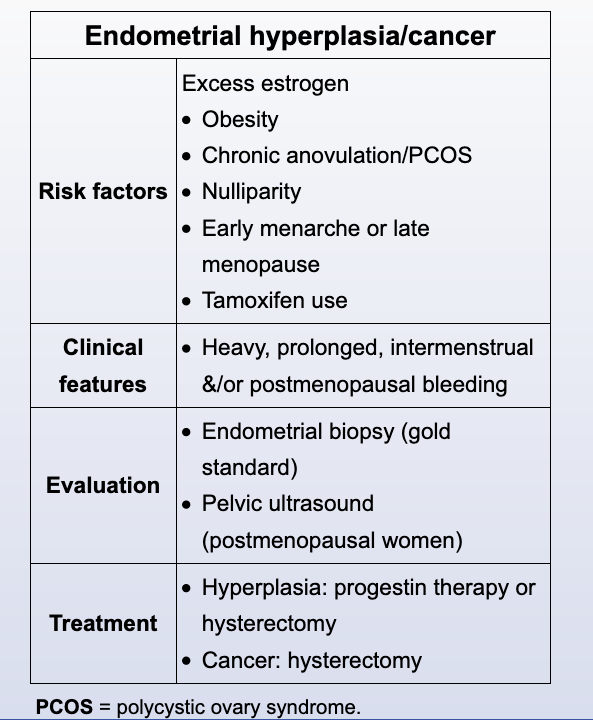
Uterine fibroids typically present with heavy, regular menstrual bleeding. This patient's intermenstrual bleeding and sudden onset of heavy, prolonged menses are atypical of fibroids and concerning for another etiology, particularly endometrial cancer. She also has multiple risk factors for endometrial cancer, including obesity, diabetes mellitus, and hypertension. Other risk factors include a history of polycystic ovary syndrome, tamoxifen use, and a history of heritable genetic disorders (eg, Lynch syndrome). Women age <45 with abnormal uterine bleeding and risk factors for endometrial cancer require evaluation of the endometrial lining with an endometrial biopsy (EMB). If the EMB is normal, the uterine fibroids can be treated with either hormonal therapy (eg, oral contraceptives) or surgical intervention (Choices D and E).
Uterine bleed

Anovulation is common during the first few years of menarche and can cause irregular, heavy menstrual periods. In the absence of ovulation, menstrual cycles lack their regular periodicity. The endometrium builds up under the influence of estrogen; however, without the influence of progesterone, the cue to slough the endometrium is lacking and menstrual-like bleeding occurs due to estrogen breakthrough bleeding. Therefore, patients often present with prolonged vaginal bleeding with passage of blood clots; initial evaluation includes assessing hemodynamic stability and estimating the volume of blood loss.
Treatment of an acute, heavy bleeding episode in hemodynamically stable patients (eg, mild anemia, no coagulation abnormalities) involves endometrial stabilization via hormonal therapy. Estrogen promotes hemostasis through further proliferation of the disordered endometrium and repairing the bleeding sites. First-line treatment is with combination oral contraceptives with high-dose estrogen. Intravenous conjugated estrogen is used in patients who either cannot tolerate oral medications or continue to bleed despite oral therapy (Choice A).
(Choice B) In a dilation and curettage, the endometrium is surgically removed to stop acute bleeding in hemodynamically unstable patients whose bleeding has not improved with intravenous estrogen or have contraindications to medical management (eg, thromboembolism). This patient is hemodynamically stable and has no contraindications to estrogen therapy.
(Choice C) An endometrial ablation is used to treat heavy, ovulatory menses in premenopausal women by destroying and removing the endometrium. This procedure is contraindicated in patients who desire future fertility, as endometrial ablation is associated with multiple obstetric complications (eg, placenta accreta, premature birth, perinatal mortality).
(Choice D) Progestin-containing implants are used for contraception. They are not indicated in the management of an acute bleeding episode due to the slow onset of action and irregular bleeding associated with initial use.