Rh Autoimmunization
- Keywords:: Step 3 Hematology
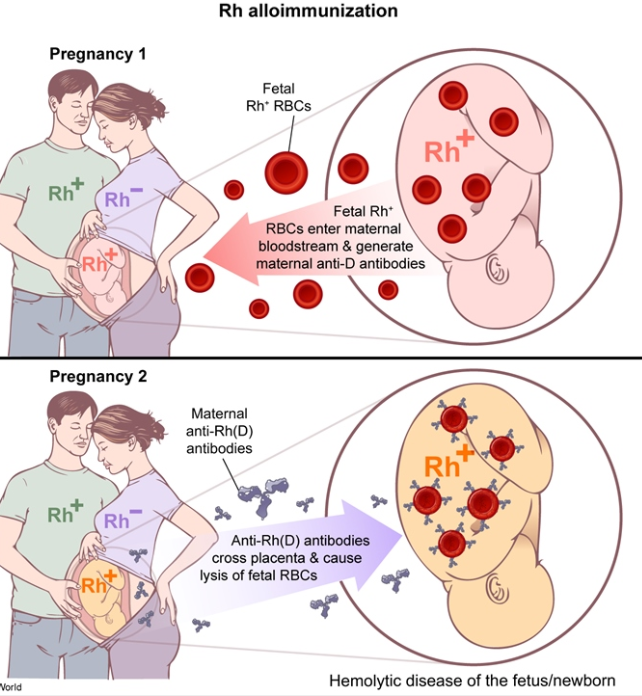
Rh(D) alloimmunization occurs when an Rh(D)-negative mother develops antibodies against Rh(D) antigen. Alloimmunization can lead to hemolytic disease of an Rh(D)-positive newborn and/or fetus; maternal IgG anti-D antibodies cross the placenta and destroy fetal red blood cells. When severe anemia develops in the fetus, it can lead to heart failure and subsequent hydrops fetalis (eg, pleural or pericardial effusion, ascites).
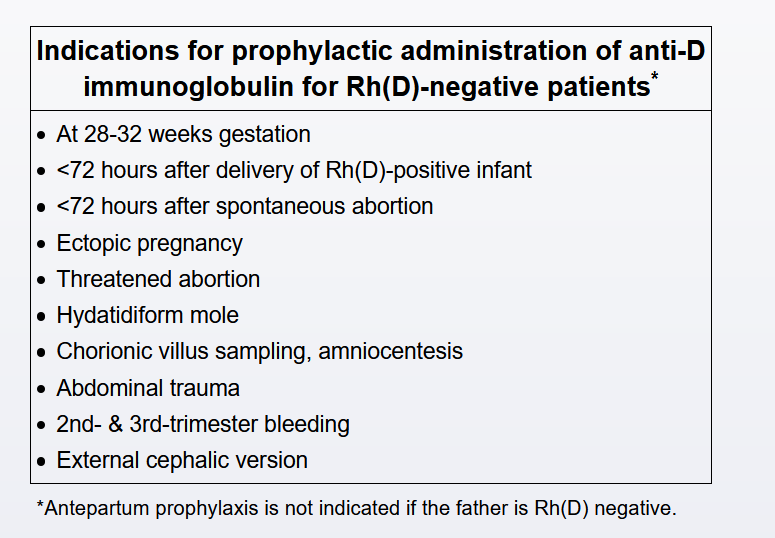
Therefore, antibody screening is performed in all pregnant women at the first prenatal visit and at 28 weeks gestation to identify antibodies that increase the risk of hemolytic disease (typically anti-D). Positive antibody screening indicates that alloimmunization has already occurred, and anti-D immune globulin is not administered. Negative anti-D antibody screening confirms a lack of antigen exposure and is an indication to proceed with anti-D immune globulin prophylaxis at 28 weeks gestation. This prophylactic anti-D immune globulin neutralizes any occult Rh(D) antigen exposure that may occur between the third trimester and delivery. The postpartum dose of anti-D immune globulin, administered <72 hours after delivery, reduces the risk of alloimmunization from fetomaternal hemorrhage associated with delivery. The postpartum dose, with the addition of the antenatal dose at 28 weeks gestation, reduces the risk of alloimmunization to <1%.
Typically, a standard 300 µg anti-D immune globulin dose is administered at 28 weeks gestation and again <72 hours postpartum in an Rh(D)-negative mother with a Rh(D)-positive infant. However, pregnancies complicated by massive fetomaternal hemorrhage (eg, abruptio placentae) may require adjustments in the anti-D immune globulin dose, as the standard dose of anti-D immune globulin prevents maternal sensitization only up to 30 mL of fetal blood. In cases of fetomaternal hemorrhage, the amount of fetomaternal transfusion is calculated, so that an adequate dose of anti-D immune globulin can be administered within the 72-hour timeframe.
The rosette test is a qualitative screening that determines the presence of fetomaternal hemorrhage. If negative, the standard dose of anti-D immune globulin is administered. If positive, the amount of hemorrhage can be determined using a Kleihauer-Betke test or flow cytometry, and the dose of anti-D immune globulin is increased based on the percentage of fetal red blood cells in the maternal circulation.