Mixed Connective Tissue Disease
- related: Rheumatology
- tags: #rheumatology
Overview
Despite long-standing attempts to define rheumatologic diseases according to precise classification, some patients express only nonspecific, nondiagnostic signs and symptoms (undifferentiated connective tissue disease UCTD), whereas others experience features of more than one disease simultaneously (overlap syndromes).
Mixed connective tissue disease (MCTD) is a specific overlap syndrome that includes clinical manifestations of at least two of the following: systemic lupus erythematosus (SLE), polymyositis, and systemic sclerosis. Positive anti-U1-ribonucleoprotein (RNP) antibodies are the primary laboratory feature.
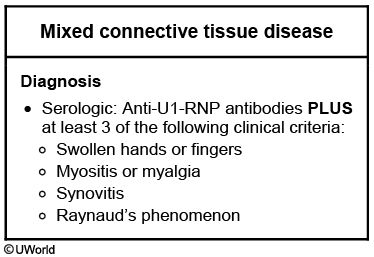
This patient’s presentation of fatigue, muscle weakness, sicca symptoms (eg, dry eyes and mouth), Raynaud’s phenomenon, and hand swelling (synovitis) is consistent with likely mixed connective tissue disease (MCTD). MCTD is an overlap syndrome associated with anti-U1-RNP (ribonucleoprotein) antibodies and features of systemic lupus erythematosus (SLE), systemic sclerosis, and polymyositis (see table above). Diagnosis usually requires at least 3 clinical criteria plus serologic criteria (see table below).
Unlike in SLE, patients with U1-RNP antibodies rarely develop diffuse glomerulonephritis, psychosis, or seizures. However, they usually develop early Raynaud’s phenomenon, sclerodactyly, inflammatory muscle disease, and pulmonary hypertension (the most common cause of death in MCTD). Patients with MCTD have a variable prognosis, with the worst prognosis for those with scleroderma and polymyositis symptoms. Treatment is usually glucocorticoids for most disease-specific manifestations.
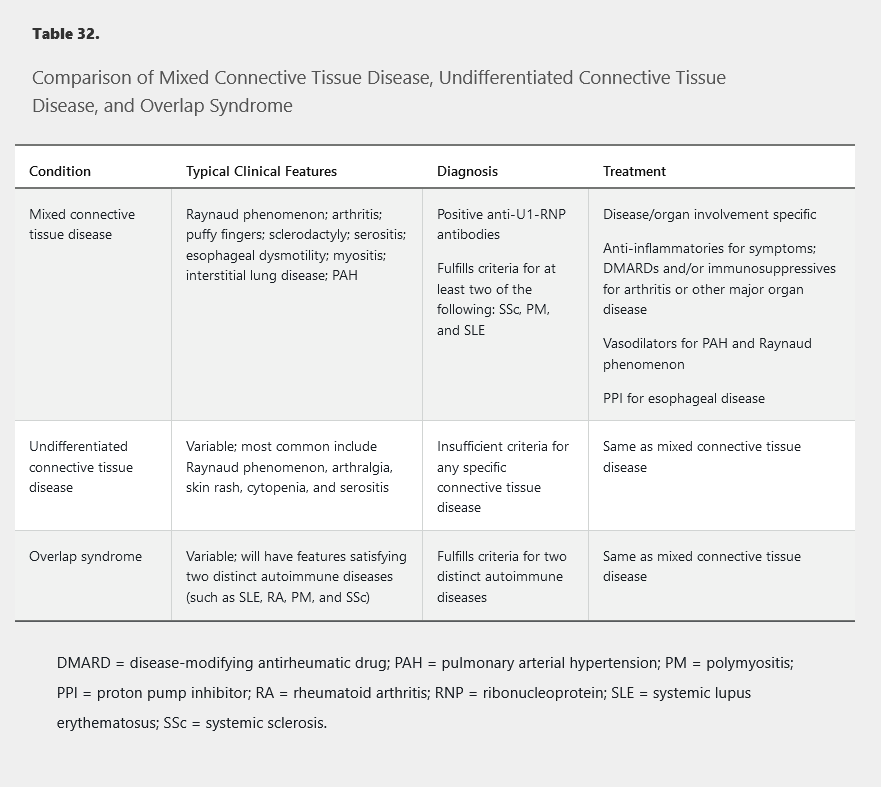
See Table 32 for a comparison of MCTD, UCTD, and overlap syndromes.
Epidemiology and Pathophysiology
MCTD is rare, and 80% of patients are women. B-cell abnormalities and an association between anti-U1-RNP antibody titer and disease activity have been described.
Clinical Manifestations and Diagnosis
See Table 32 for details on the clinical manifestations and diagnosis of MCTD. Raynaud phenomenon is a particularly common feature. Pulmonary arterial hypertension is the major cause of death, but severe kidney disease is uncommon. Although antinuclear antibodies, rheumatoid factor, and anti–cyclic citrullinated peptide antibodies are often present, the presence of anti–double-stranded DNA or anti-Smith antibodies make SLE a more likely diagnosis.
Management
Treatment for MCTD is directed at the specific diseases and organ system involvement manifesting in the individual patient (see Table 32).
Prognosis
Prognosis of MCTD varies depending on the spectrum and severity of organ involvement. Patients with initially mild disease may develop new and more severe manifestations over decades, importantly including interstitial lung disease and pulmonary arterial hypertension. As with many other systemic inflammatory disorders, patients are at increased risk of atherosclerotic cardiovascular disease.
UCTD usually remains mild and stable but over time may evolve into a more specific autoimmune disorder, most commonly SLE.