Mitral regurgitation surgical indications
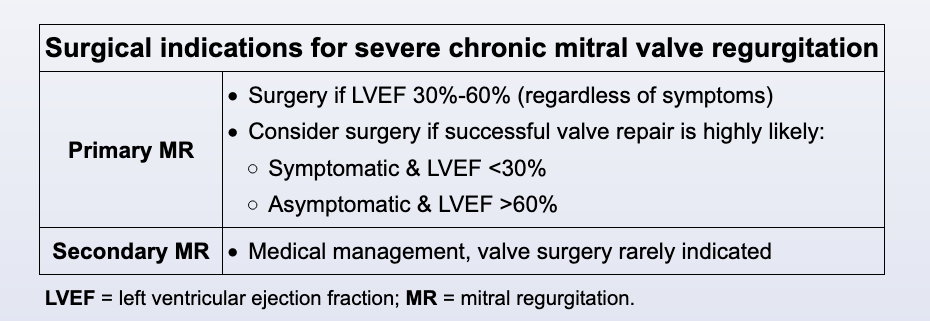
Primary mitral valve regurgitation (MR) is defined as MR caused by an intrinsic defect of the mitral valve apparatus (eg, leaflets, chordae tendineae) and is differentiated from secondary MR, which results from other cardiac disease (eg, myocardial ischemia, dilated cardiomyopathy). This patient's echocardiogram reveals severe, chronic primary MR, which is likely due to myxomatous degeneration of the mitral valve. Atrial fibrillation (AF) due to left atrial dilation is a common complication of severe MR.
A large portion of the left ventricular ejection fraction (LVEF) flows back into the left atrium in patients with severe MR; therefore, the effective LVEF is much lower than estimated by echocardiogram. As a result, in order to prevent irreversible loss of left ventricular function, surgery is recommended for both symptomatic and asymptomatic patients with severe, chronic primary MR and LVEF 30%-60%; mitral valve repair is preferred over replacement whenever possible. Patients with LVEF <30% likely have life-limiting, permanent systolic dysfunction, and surgery is deemed worthwhile only when there is a high likelihood of successful and durable valve repair (rather than replacement). Preemptive surgery is indicated in asymptomatic patients with LVEF >60% who are excellent candidates for successful and durable valve repair.
Medical therapy is of limited utility in patients with severe primary MR. When necessary, typical heart failure medications (eg, ACE inhibitors, beta blockers, diuretics, aldosterone antagonists) are used, but surgery is the only proven and definitive therapy.
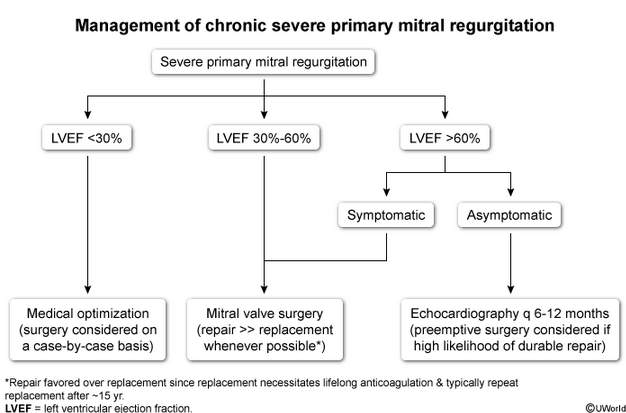
This patient has mitral valve prolapse with severe mitral regurgitation (MR). Once chronic primary MR becomes severe, it is definitively managed with mitral valve surgery; whenever possible, valve repair is favored over replacement because replacement necessitates lifelong anticoagulation and typically repeat replacement after approximately 15 years. Guidelines seek to optimize the timing of surgery such that patients obtain full usage of their native valve without developing irreversible left ventricular systolic dysfunction. The surgical timing is largely based on left ventricular ejection fraction (LVEF):
- LVEF <30%: Many of these patients have irreversible left ventricular dysfunction that will not significantly improve with surgery. Surgery should be considered on a case-by-case basis.
- LVEF 30%-60%: Surgery is indicated for all patients, regardless of symptoms. A high-end cutoff of 60% is in place because LVEF overestimates forward stroke volume in patients with severe MR.
- LVEF >60%: Surgery is indicated for symptomatic patients. For asymptomatic patients (such as this one), monitoring with echocardiography every 6-12 months is usually recommended. Preemptive valve repair can be considered in asymptomatic patients with very high likelihood of durable valve repair and may be appropriate in this patient; in contrast, valve replacement (vs repair) is inappropriate because it would substitute a still viable native valve for a prosthetic valve requiring lifelong anticoagulation. Replacement is appropriate only when there is a firm surgical indication and repair is not possible (Choice D).
Other surgical indications for asymptomatic patients with LVEF >60% include an enlarged left ventricular end-systolic diameter >40 mm, pulmonary artery systolic pressure >50 mm Hg, or new-onset atrial fibrillation, none of which are present in this patient.