EBV
- related: CNS lymphoma
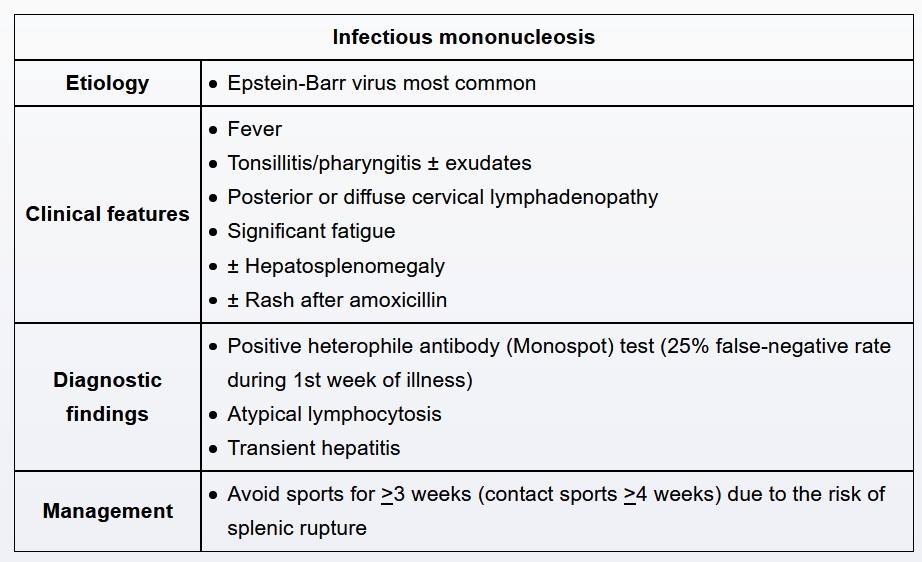
Epstein-Barr virus (EBV) is the most common causative agent of IM and is transmitted via contact with oropharyngeal secretions. The diagnostic test of choice in confirming EBV IM is the heterophile antibody test, which screens for IgM antibodies called heterophile antibodies. These antibodies are produced in response to EBV infection and agglutinate with erythrocytes from unrelated species (eg, horse erythrocytes in the Monospot test, sheep erythrocytes in the classic Paul-Bunnell test). Atypical lymphocytes are often seen on peripheral blood smears but are not specific for IM.
Corticosteroids are warranted in the treatment of infectious mononucleosis (IM) in rare cases when airway obstruction appears imminent; common warning signs include shortness of breath while recumbent, tachypnea, and inability to swallow. Corticosteroids may also be considered in patients with IM who are immunocompromised or are experiencing other serious complications (eg, aplastic anemia, overwhelming infection, thrombocytopenia).
Primary HIV infection should be suspected in a sexually active individual with unexplained fever, fatigue, weight loss, and lymphadenopathy. However, exudative pharyngitis is not seen in HIV infection, whereas symptoms such as diarrhea and rash usually are.
Although this patient meets some of the Centor criteria (ie, fever, exudative pharyngitis, lack of cough), streptococcal pharyngitis is unlikely in a patient with generalized lymphadenopathy and hepatosplenomegaly.