Barrett's
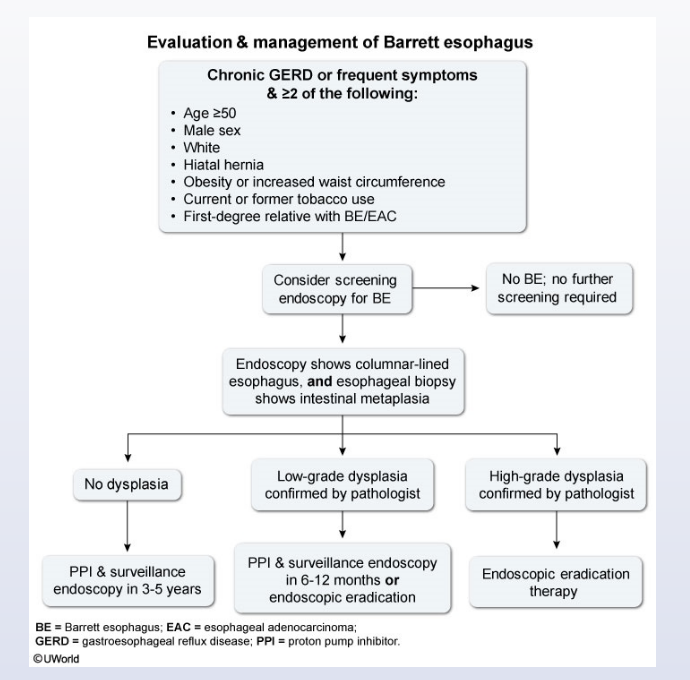
Most guidelines suggest a screening endoscopy in patients with frequent gastroesophageal reflux disease (GERD) symptoms and ≥2 risk factors for Barrett esophagus (eg, age ≥50, male sex, tobacco use).
Esophageal biopsy (4-quadrant biopsies within every 2 cm) is performed in patients with visual evidence of intestinal metaplasia on endoscopy. Patients with intestinal metaplasia without dysplasia on pathologic evaluation can undergo surveillance endoscopy in 3-5 years. Patients with low-grade dysplasia require surveillance endoscopy every 6-12 months or endoscopic eradication therapy (eg, ablation, mucosal resection). High-grade dysplasia is an indication for endoscopic eradication therapy.
This patient has Barrett esophagus without dysplasia and requires surveillance endoscopy in 3-5 years. Because there is no high-grade dysplasia, he does not need endoscopic ablative therapy or mucosal resection (Choice A). Proton pump inhibitor (PPI) therapy can decrease the patient's symptoms, heal the esophagitis, and may slow the progression of Barrett esophagus to cancer.