rhabdomyolysis
- related: MSK
- tags: #msk
This patient with a recent stroke, who was found confused and incontinent, has developed acute kidney injury (AKI); urinalysis shows 4+ blood in the absence of red blood cells (RBCs). This presentation suggests rhabdomyolysis likely due to seizure.
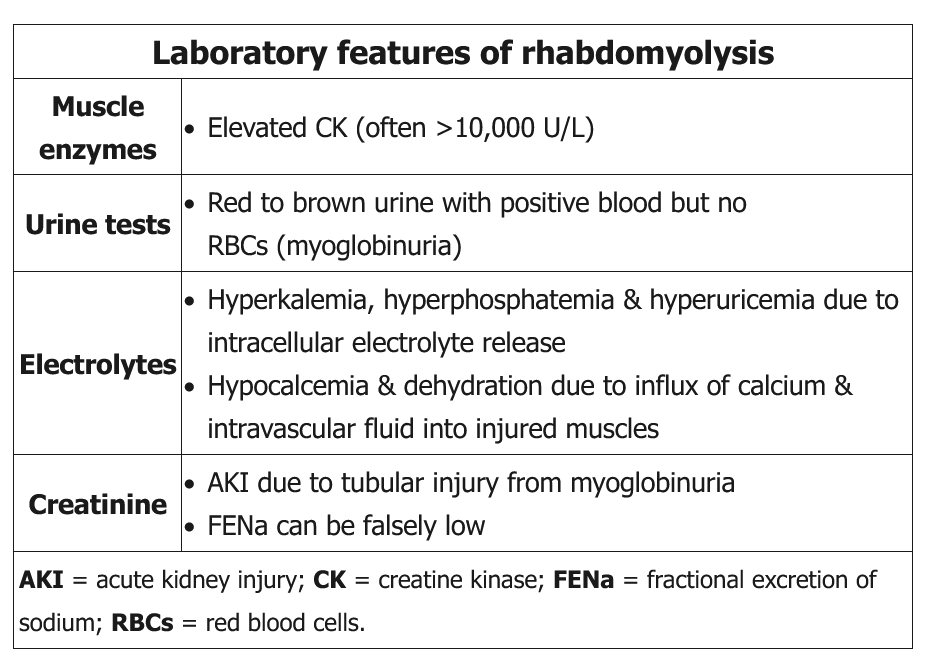
Rhabdomyolysis is characterized by the release of intracellular muscle contents into the circulation after muscular injury; it is common with crush injuries, prolonged muscle activity (eg, seizure, excessive exercise), or drug use (eg, phencyclidine). Positive blood on urine dipstick (a reaction that detects the iron-containing heme pigment in both hemoglobin and myoglobin) in the absence of RBCs (<3/hpf) on microscopic urinalysis suggests myoglobinuria.
AKI in rhabdomyolysis typically results from an abundance of filtered heme-pigment leading to acute tubular necrosis; however, the fractional excretion of sodium (FENa) is often unexpectedly low (<1%) despite the intrinsic renal injury that occurs, possibly due to renal vasoconstriction. Hyperkalemia, hyperphosphatemia, and hyperuricemia are predominantly due to muscle cell lysis and are often disproportionate to the degree of renal failure. Markedly elevated serum creatine kinase (often >10,000 U/L) confirms the diagnosis.
This patient with a seizure from phencyclidine (PCP) has urinalysis evidence of blood with minimal red blood cells, raising suspicion for myoglobinuria due to rhabdomyolysis.
Rhabdomyolysis is characterized by the release of intracellular muscle components into the circulation after muscular injury. Most cases arise due to trauma, compression injury, infection, drug use (eg, PCP), or toxin exposure. Diagnosis is typically made when laboratory results show markedly elevated creatine kinase levels (usually >10,000 U/L). Urinalysis often reveals blood with no red blood cells, indicating myoglobinuria.