prolactinoma
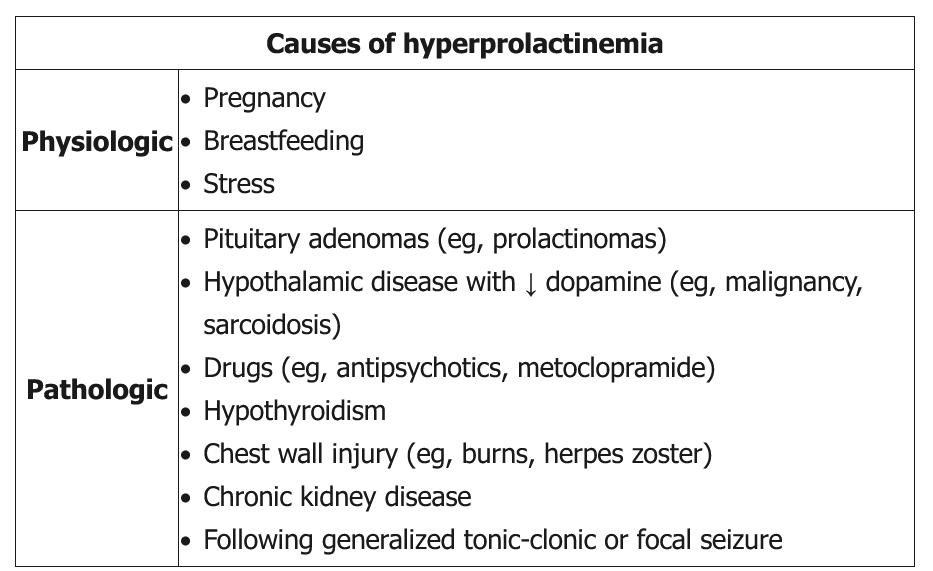
Prolactin levels naturally increase during pregnancy due to stimulation from high estrogen levels, peak at delivery, and then normalize within 1-2 months after delivery, even with continued breastfeeding. Although prolactin levels increase transiently above basal levels with response to suckling, this response significantly diminishes a few weeks after delivery. This patient is no longer breastfeeding and is not currently taking any medications (eg, antipsychotics) that would explain increased prolactin levels.
The most likely cause of this patient's elevated prolactin is a prolactinoma (ie, lactotroph adenoma). Prolactinomas can present with secondary amenorrhea, bilateral milky nipple discharge (ie, galactorrhea), and hypogonadism. A significantly elevated prolactin (>200 ng/mL) level usually indicates a prolactinoma. In any patient who has hyperprolactinemia and is not taking any medication known to increase prolactin levels, an MRI of the head should be performed to screen for a pituitary mass (Choice D). Additional evaluation of prolactinomas includes formal visual field testing due to the potential for the pituitary mass to compress the optic chiasm.
Prolactinomas that cause hypogonadism (eg, amenorrhea) or neurologic symptoms (eg, headaches, visual disturbances) secondary to mass effect are treated first-line with dopamine agonists (eg, cabergoline, bromocriptine) and followed with serial MRIs. Surgery (eg, transsphenoidal resection) is reserved for patients who fail medical therapy.
Male patients with atrophic testes, decreased sexual performance, and an elevated serum prolactin level have a prolactinoma until proven otherwise. Brain MRI in this patient is likely to reveal a mass in the pituitary gland. His visual field deficit is further suggestive of a pituitary mass, as bitemporal hemianopsia can result from compression of the optic chiasm. A prolactinoma is a benign neoplasm of the lactotroph cells in the pituitary gland. In men, the hyperprolactinemia induced by this tumor results in a decreased serum testosterone concentration, which can cause decreased libido, muscle mass, body hair, and testicular size.
Patients with a prolactinoma need to be treated if they meet either of the following criteria: presence of neurologic symptoms secondary to the size of the mass, or hypogonadism or other symptoms secondary to hyperprolactinemia. Initial treatment should consist of a dopamine agonist such as cabergoline or bromocriptine; in >90% of patients, pharmacologic management decreases prolactin secretion and reduces the size of the mass. Surgery should be reserved for patients who do not respond to dopamine agonist therapy.