Hyperthyroidism
- related: Endocrine
- tags: #note
Sx
- tachycardia
- AMS, psychosis, agitation, anxiety
- lid lag, stare, itchy eyes
- hyperreflexia
Dx
- high output cardiac failure
- all types of tachyarrhythmias
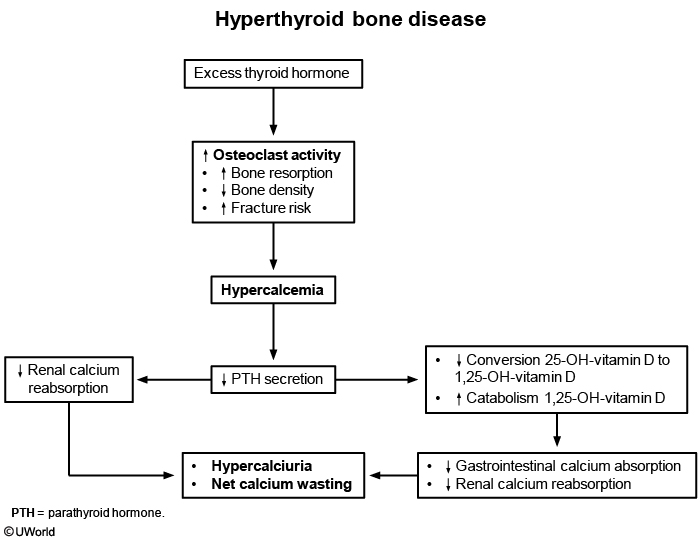
- hypercalcemia
- elevated LFTs
- thrombocytopenia
- TSH, free T4, total T3
Treatment
- work up for inciting events: infection, DKA, pancreatitis
- beta blocker
- Methimazole
- Others
- steroids
- high dose iodine: can use up to 5 days to stop thyroid hormone production
- cholestyramine: reduce recycling
- rarely plamaphresis: remove thyroid stimulating abx, protein bound thyroid hormones
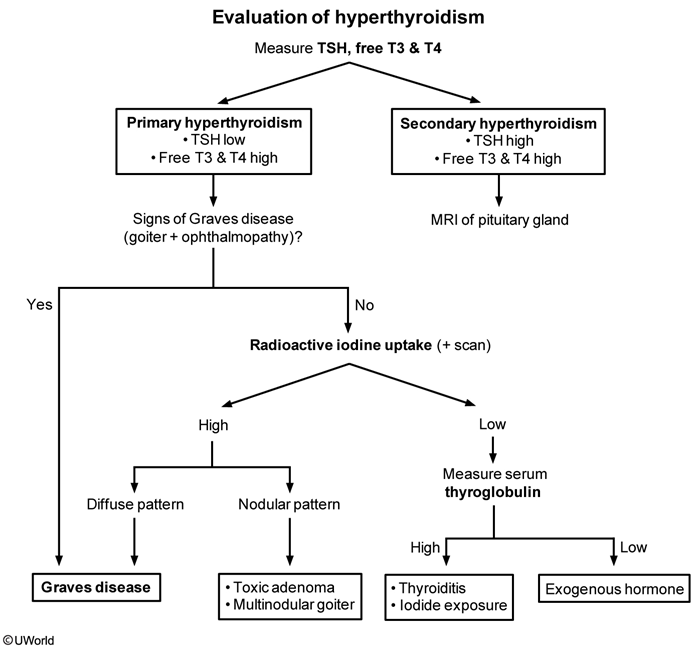
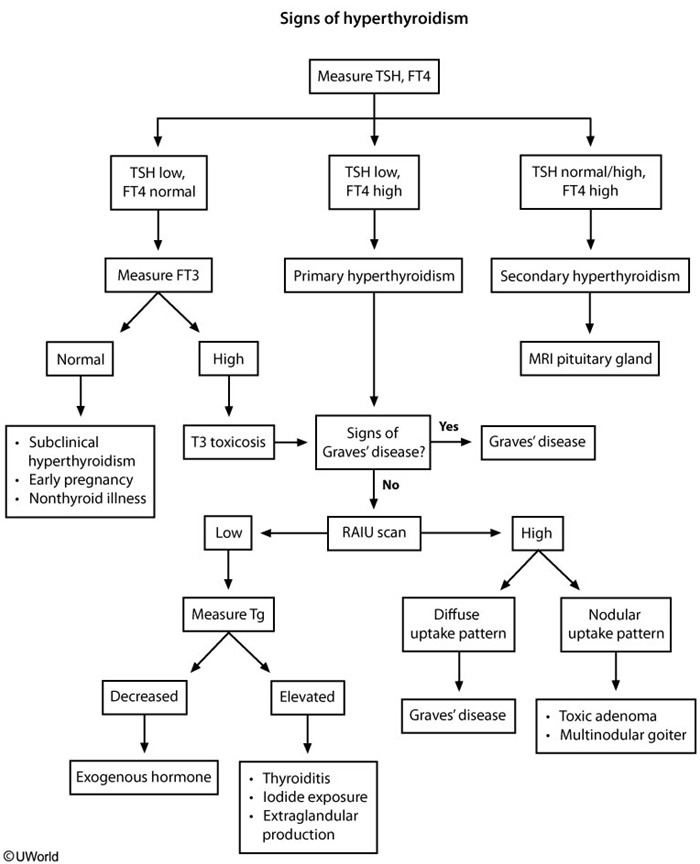
Workup for exogenous thyrotoxicosis
This patient has hyperthyroidism with tachycardia, tremor, and elevated free T4. She has no goiter or extrathyroidal manifestations (eg, proptosis) of Graves disease and no palpable nodules to suggest toxic nodular disease. In light of the association between the over-the-counter "energy" pills and the onset of symptoms, it is likely this patient has exogenous thyrotoxicosis due to desiccated thyroid extracts. Bovine and porcine thyroid supplements can be obtained without a prescription and have been promoted for weight loss and increased energy. Exogenous thyrotoxicosis can also be caused by excessive or surreptitious dosing of prescription thyroid medication.
In the evaluation of exogenous thyrotoxicosis, 2 tests are helpful:
- The 24-hour radioactive iodine uptake (RAIU) is low with exogenous thyrotoxicosis as thyroid extracts suppress thyroid follicular activity. Other causes of hyperthyroidism with a low RAIU include inflammatory thyroiditis and, rarely, ectopic thyroxine production (eg, struma ovarii).
- If RAIU is low, thyroglobulin levels should be checked. With exogenous thyrotoxicosis, the concentration of thyroglobulin (released in small amounts by normal thyroid follicles) is also low due to suppressed follicular activity. Elevated serum thyroglobulin levels can be seen in patients with increased follicular activity (eg, Graves disease) or follicular injury (eg, thyroiditis).