Concussion
Concussion is a mild traumatic brain injury caused by axonal shearing from rapid rotational acceleration of the brain during a fall or strike to the head. Children and adolescents playing contact sports (eg, soccer) are at increased risk for concussions.
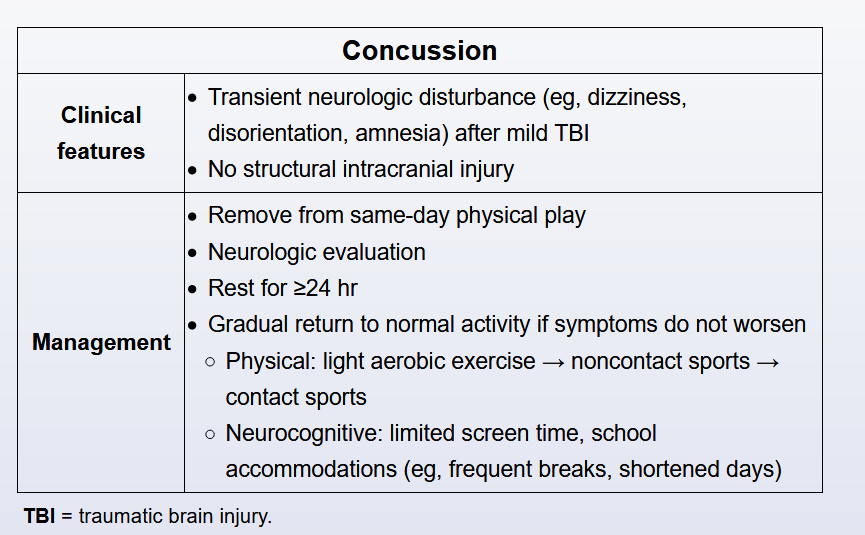
Patients are usually diagnosed clinically based on the presence of a neurologic disturbance (eg, headache, cognitive dysfunction) after head trauma. Neuroimaging is not typically required unless high-risk features for structural intracranial injury are present (ie, altered mental status, loss of consciousness, severe headache/vomiting, severe mechanism of injury, signs of basilar skull fracture).
Initial management is physical and cognitive rest for 24-48 hours. Athletes should then follow a gradual return-to-play protocol with progressive intensity of physical exercise (eg, light aerobics → moderate noncontact activity → competitive play) as tolerated. If symptoms worsen at any level of exertion, a 24-hour rest period is recommended before returning to the previous step in the protocol that did not exacerbate symptoms.
In this case, the patient tolerated light aerobics but developed dizziness and nausea with moderate exercise; therefore, she should rest for a day and then return to light aerobic activity.
Brain imaging to exclude structural intracranial injury may be considered for worsening symptoms despite appropriate rest and adherence to the gradual return-to-play protocol. In contrast, this patient's symptoms that wax and wane with exertion are typical of a concussion and can be managed by adjusting the activity level.