autoPeep
- related: Pulmonology
- tags: #pulmonology
In a mechanically ventilated patient, positive end-expiratory pressure (PEEP) can be divided into extrinsic and intrinsic components. The extrinsic component is that provided by the ventilator; the intrinsic component is that caused by air remaining in the lungs due to incomplete expiration. Patients with obstructive lung disease (eg, asthma, chronic obstructive pulmonary disease) are at increased risk of excessive accumulation of intrinsic PEEP (auto-PEEP) as they are unable to complete exhalation before the start of the next inspiratory cycle. As this occurs over repeated breaths, end-expiratory alveolar pressure rises above the extrinsic PEEP and results in auto-PEEP.
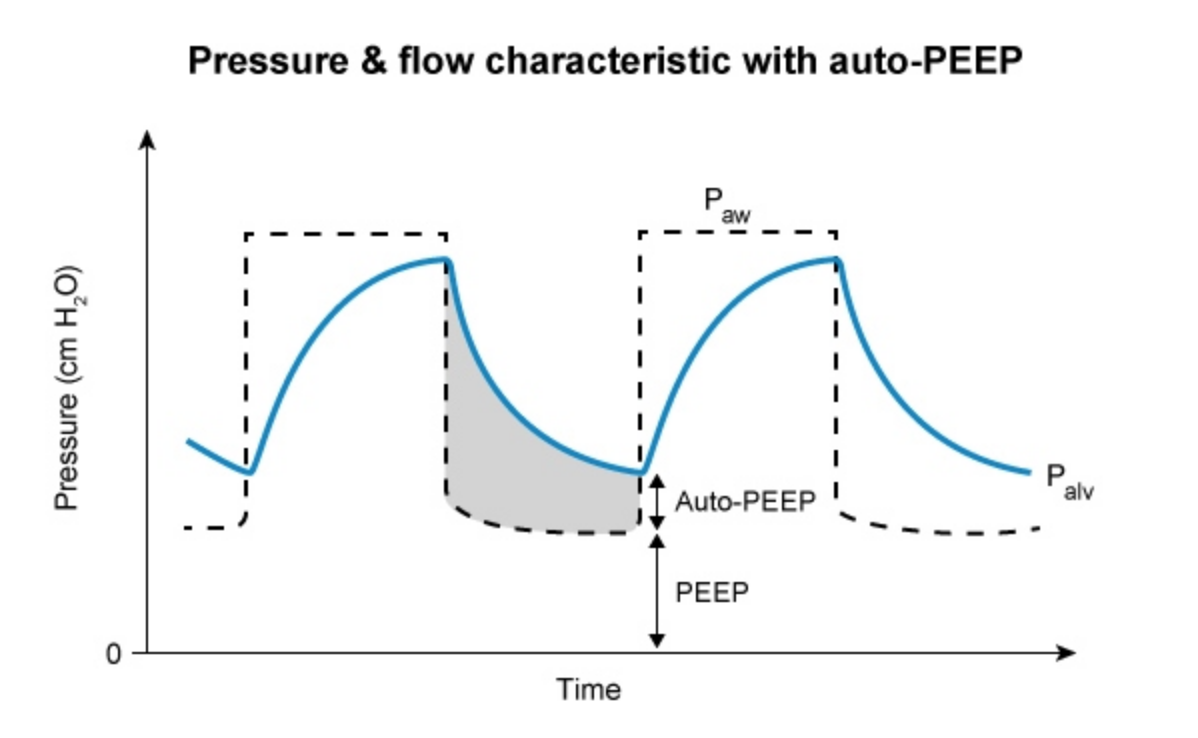
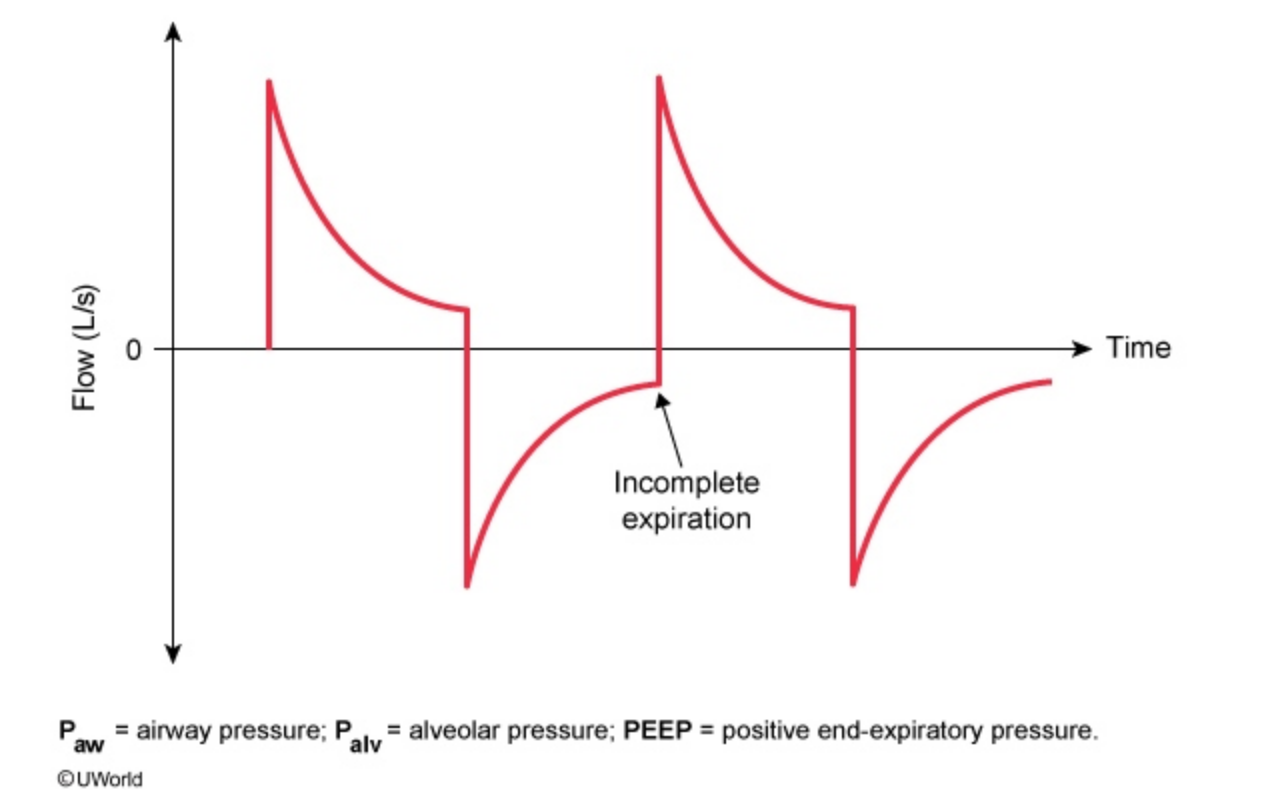
On ventilatory waveforms, this phenomenon is demonstrated by air flow that does not return to zero before the next breath initiates. Auto-PEEP causes alveolar distension, increasing the risk for ventilator-associated lung injury. Strategies for correcting auto-PEEP include reducing minute ventilation (reduction in tidal volume or respiratory rate), increasing expiratory time, and using bronchodilators and inhaled corticosteroids to relieve airway obstruction. In addition, increasing the extrinsic PEEP can be helpful in treating auto-PEEP by reducing the pressure threshold for initiating a new breath and better distributing inspired air.