Hypertension
- elderly patients have lower blood pressure goal
- nsaid use can increase blood pressure
- secondary HTN
- inpatient hypertension
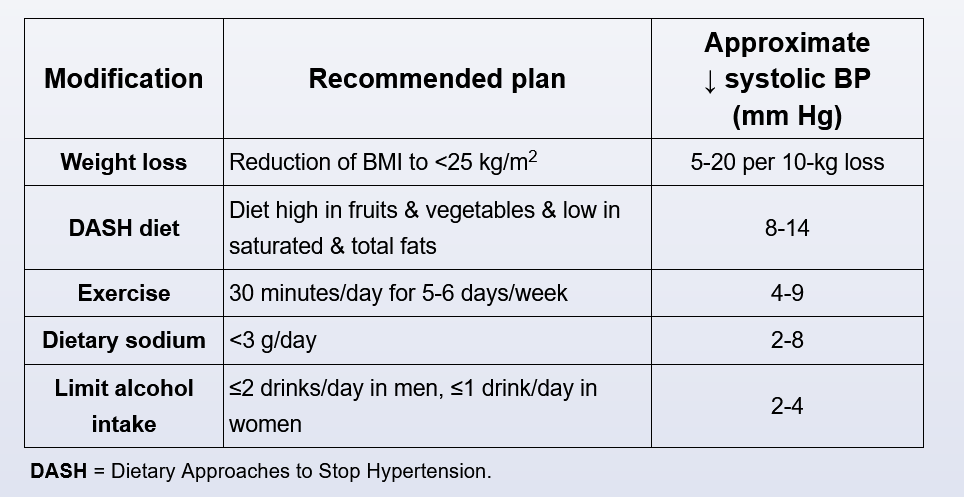
BP lowering
Transplant HTN
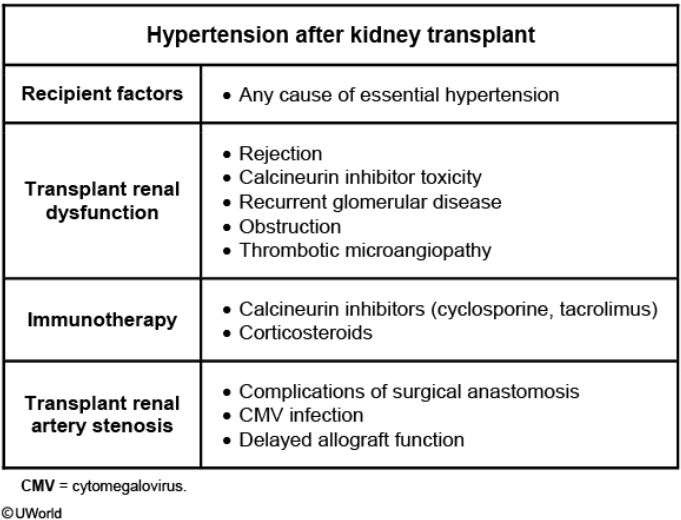
About 90%-95% of patients with a kidney transplant have hypertension secondary to specific transplant-related factors or recipient characteristics. This patient presents with severe hypertension and normal baseline renal function (creatinine of 1.1 mg/dL), which is unlikely to be seen in allograft rejection. This patient developed acute kidney injury (creatinine increased to 2.4 mg/dL) after the initiation of an ACE inhibitor. This is highly suggestive of underlying transplant renal artery stenosis as the cause of his hypertension.
Renal hypoperfusion due to renal artery stenosis stimulates the renin-angiotensin-aldosterone system that in turn causes hypertension and maintains the glomerular capillary pressure and glomerular filtration rate (GFR). In patients with bilateral renal artery stenosis or renal artery stenosis in a solitary kidney (eg, patients with transplant), administration of ACE inhibitors lowers the angiotensin II level acutely, leading to a significant decrease in GFR (by >30%) and acute kidney injury. Renal artery stenosis should also be suspected in transplant recipients with resistant hypertension, flash pulmonary edema, or progressive loss of renal function.
Transplant renal artery stenosis causes hypertension in 10%-12% of patients usually within the first 2 years after kidney transplantation. Improper surgical anastomosis is an important cause. It can also occur in acute rejection and cytomegalovirus infection.